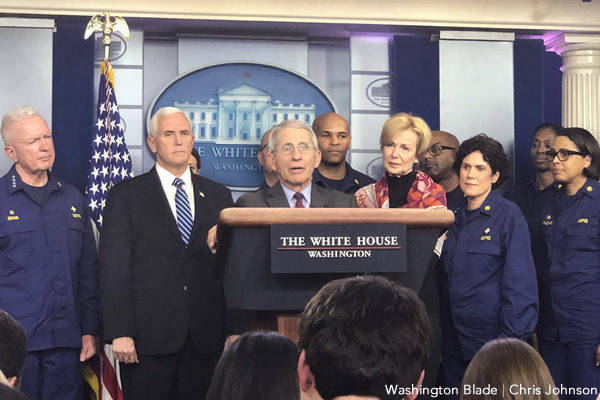
Dr. Anthony Fauci said Tuesday the visibility LGBTQ people brought to themselves during the height of the HIV/AIDS epidemic helped change the tide for public perception.
Fauci made the remarks during the daily White House Coronavirus Task Force briefing when responding to COVID-19’s disproportionate impact on black Americans, saying the disease has “shed a light” on health disparities in the United States much like HIV/AIDS did with LGBTQ people.
“During that time, there was extraordinary stigma, particularly against the gay community,” Fauci said. “And it was only when the world realized how the gay community responded to this outbreak with incredible courage and dignity and strength and activism — I think that really changed some of the stigma against the gay community, very much so.”
As head of the National Institute of Allergy & Infectious Diseases, Fauci was responsible for developing medications to treat HIV/AIDS at the height of epidemic. His efforts resulted in drugs still used today, although that came after activism of groups like ACT UP pushing the U.S. government to release the medication.
The impact of HIV/AIDS on LGBTQ people, Fauci said, is similar to the impact COVID-19 is having on African-Americans.
“When you’re in the middle of a crisis, like we are now with the coronavirus, it really does have ultimately shine a very bright light on some of the real weaknesses and foibles in our society,” Fauci said.
State data on COVID-19 is beginning to reflect African-Americans suffer from the disease at a greater rate than others.
In Michigan, for example, 35 percent of all COVID-19 cases are black or African-American, as are 40 percent of all deceased cases, according to state data. But the black or African-American population makes up just 14.1 percent of Michigan’s population.
Fauci said COVID-19’s has a disproportionate impact on black people not because they’re getting infected more often, but because the population suffers from health disparities.
“When they do get infected, their underlying medical conditions — the diabetes, the hypertension, the obesity, the asthma — those are the kind of things that wind them up in the ICU and ultimately give them a higher death rate,” Fauci said.
Fauci concluded the COVID-19 epidemic “will end,” but when that happens “there will still be health disparities which we really do need to address in the African-American community.”
President Trump expressed indignation over the disproportionate impact COVID-19 is having on the black population.
“What’s happening is we’re trying to find out why is it that it’s three and four times,” Trump said, “Now, maybe that’s not going to be the final number, but why is it three or four times more so for the black community as opposed to other people. It doesn’t make sense, and I don’t like it.”
Trump said his administration would have statistics on COVID-19’s impact on black people in “probably two to three days.”
Asked by a reporter if that pattern of black people being disproportionately affected by COVID-19 will continue nationwide, Fauci hinted that was the case.
“I can’t be confident to predict patterns, but the underlying reason why that is happening doesn’t change from state to state,” Fauci said. “I expect that when African-Americans get infected, given the disproportionate disparity of the underlying conditions that lead to complications like the ones I mentioned, I expect that we will still see the pattern that when you loo at the proportion of people who get into serious trouble and die, again, it’s going to be disproportionate towards the African-Americans. I do expect.”
Fauci affirmed the federal government is now leading the charge in collecting information said it will be public in days or the coming week.
Although states are collecting information on the racial and ethnic identities of COVID-19 patients, they aren’t ascertaining whether patients are LGBTQ. The lack of information has angered LGBTQ advocates, who are calling for greater data collection because LGBTQ are vulnerable to COVID-19.
Faced with tremendous pressure during the coronavirus crisis to lift its policy barring gay men from donating blood, the Food & Drug Administration announced on Thursday it has eased the restrictions.
While the previous policy, established in 2015, barred men who have had sex with men in the 12 months from making a donation, the new policy would shorten the deferral period, requiring abstinence for only three months.
The FDA indicated it would make a change in a notice to stakeholders on Thursday, indicating the decision was based on “evaluation of the totality of the scientific evidence available.”
“To help address this critical need and increase the number of donations, the FDA is announcing today that based on recently completed studies and epidemiologic data, we have concluded that the current policies regarding the eligibility of certain donors can be modified without compromising the safety of the blood supply,” the notice says.
In addition changing the recommended deferral period for men who have had sex with men from 12 months to 3 months, the FDA informs stakeholders of other changes.
Among them are easing ban on donations for women who have had sex with men who, in turn, previously have had sex with a man. For these women the deferral period has similarly been changed from 12 months to 3 months.
Further, the new policy eases recommended 12 month deferral for individuals with recent tattoos and piercings to three months, and eases from an indefinite ban to a three month ban for donations from people who have a past history of sex in exchange for money, or injection drug use.
Other changes are implemented easing policy related to blood donors who have travelled to malaria-endemic areas, such as countries in Africa, or to European countries where the donors faces potential risk of transmission of Creutzfeldt-Jakob Disease or Variant Creutzfeldt-Jakob Disease.
The FDA issued the notice to stakeholders at the same time it published on its website a 17-page official memo outlining the changes, declaring they were made to address the shortage in the blood supply amid the COVID-19 crisis and therefore would not wait for a public comment period.
“As a result of this public health emergency, there is a significant shortage in the supply of blood in the United States, which early implementation of the recommendations in this guidance may help to address (even though the recommendations in this guidance are broadly applicable beyond the COVID-19 public health emergency),” the memo says.
The three month deferral period is consistent with recommendations from the American Red Cross, which before the coronavirus had called on the FDA to shorten the deferral period.
Amid the coronavirus crisis, state health officials responsible for gathering data on COVID-19 are declining to collect and report whether or not patients identify as LGBTQ — a practice that angers LGBTQ advocates who say those answers could yield important information to combat the disease.
The lack of data, advocates say, will essentially blind the public to the coronavirus’ impact on LGBTQ people — a population that may be particularly vulnerable to COVID-19 — as the epidemic continues to rise and health officials warn the death toll in the United States will hit its peak in the coming weeks.
An estimated 100,000 to 240,000 Americans may die as a result of the coronavirus epidemic, U.S. government health advisers said this week.
The deputy director of the National LGBT Cancer Network, who goes by the name Scout and has a Ph.D. in sociomedical sciences from Columbia University, said the lack of data on the coronavirus’ impact on LGBTQ people reflects the absence of LGBTQ data collection in medical surveys writ large.
“The common phenomenon of not collecting LGBTQ health surveillance data hurts us in so many ways. Now it will hurt us by masking the impact of COVID-19 on our communities,” Scout said. “Considering an estimated 3.3 million of us use tobacco products, and therefore have a higher risk of negative outcomes if we get coronavirus, not collecting LGBTQ+ status in health surveillance data is horrible. We will mourn our losses but never be able to measure them.”
The Blade reached out to several states where the confirmed cases of coronavirus infection are at their highest and as of this week surpassed 5,000 cases, according to data from the Centers for Disease Control & Prevention. Additionally, the Blade sought LGBTQ demographic information on the COVID-19 impact from jurisdictions local to the D.C. region and states that have had greater incident rates of COVID-19 cases.
The only jurisdiction to report having collected data on whether COVID-19 patients identify as LGBTQ was D.C,, where the department of health affirmed Tuesday to the Blade that process was underway.
“DC Health is collecting information about LGBTQ+ status of coronavirus patients,” said Alison Reeves, a D.C. Department of Health spokesperson. “However, that data is incomplete and will not be made public at this time.”
Harper Jean Tobin, director of policy for the National Center for Transgender Equality, said any reporting on COVID-19’s impact on LGBTQ people would likely be an undercount “due to the fast spread of the virus and the extraordinary shortcomings in the United States’ response to the pandemic.”
“Unfortunately, many of our pre-existing public health surveillance systems did not yet incorporate basic demographic data about LGBTQ people, and many health care institutions haven’t yet implemented this data collection in their patient record systems either,” Tobin said. “That’s inexcusable, but it’s also not likely we’ll be able to correct those deficiencies in the middle of a fast-moving global pandemic.”
Jurisdictions other than D.C. either didn’t respond to the Blade’s request to comment, or affirmed they didn’t collect data on whether coronavirus patients identify as LGBTQ.
In Michigan, where Detroit has become a new epicenter for the coronavirus epidemic, a spokesperson for the state department of health confirmed LGBTQ status of patients isn’t asked by health officials.
“That’s not something captured in the Michigan Disease Surveillance System where cases are reported, so we wouldn’t be able to determine that information,” said Lynn Sutfin, a spokesperson for Michigan Department of Health and Human Services.
The Michigan Department of Health and Human Services didn’t respond to a follow-up email inquiry on why LGBTQ status isn’t collected in the state medical data system.
In New York, a spokesperson said the NY Department of Health is “not tracking COVID-19 cases by sexuality,” then when asked why that was the case referred the Blade to recent remarks from Gov. Andrew Cuomo on COVID-19.
“This virus does not discriminate,” Cuomo said. “It doesn’t discriminate by age. It doesn’t discriminate by party. It affects all Americans, and what you’re seeing in New York is going to spread across this country.”
Privacy issues around asking COVID-19 patients whether they identify as LGBTQ were cited by one state contacted by the Blade about LGBTQ demographics on the epidemic.
In Washington State — where the coronavirus spread early on the during the epidemic, but has since stabilized compared to other states — the state department of health affirmed it doesn’t collect data on whether coronavirus patients identify as LGBTQ.
Danielle Koenig, a Washington State Department of Health spokesperson, said, “We don’t have sexual orientation information on patients.” When asked why that was the case, Koenig replied, “We don’t publish more specific demographic data to protect patient privacy.”
Tobin sought to assuage concerns about privacy issues on collecting LGBTQ information in health surveys by saying state officials could keep it confidential and that information could be used to augment health care.
“Providers and our leaders need to make sure that everyone who needs help is getting it, and discrimination won’t be tolerated,” Tobin said. “Though it may take much longer than it should, we need to ensure going forward that LGBTQ-inclusive demographic data is included in all our health surveillance and electronic health record systems, that this information is voluntary and confidential, and that it’s used to improve access and quality of care.”
The departments of health for New Jersey, Maryland and Virginia didn’t respond to the Blade’s request to comment, and the California Department of Health referred the Blade to a page on its website showing the information state officials record for COVID-19. (It doesn’t include whether patients identify as LGBTQ.)
Emphasizing changing forms to include LGBTQ questions amid a pandemic may not be realistic, Tobin cited several examples for why they would have been useful, including finding out whether LGBTQ people have particular health vulnerabilities and the right way to tailor public health messages.
“The health care system runs on data,” Tobin said. “Collecting information in patient records helps promote honest communication between patients and staff to make sure their health needs and concerns are addressed. It helps us determine whether certain populations are seeking or receiving specific services at different rates, or having different outcomes.”
The lack of data collection on whether coronavirus patients identify as LGBTQ appears to be the result of a general practice as well as the official CDC form specific for COVID-19 data collection, which doesn’t include questions seeking to identify whether a patient is LGBTQ.
The CDC form seeks to obtain information on patients who tested positive for COVID-19 based on age, sex and ethnicity, but no where does it ask their sexual orientation.
For the query on sex, the form allows states to record the patient’s answer as “male,” “female,” “none,” or “other.” Although those options provide some flexibility to patients who are non-binary, it doesn’t explicitly seek to ascertain whether a COVID-19 patient is transgender.
The Centers for Disease Control didn’t respond to multiple requests from the Blade on whether it has information on COVID-19’s impact on LGBTQ people, nor why its data collection survey doesn’t ask patients if they identify as LGBTQ.
Tobin said she’s optimistic about seeing more LGBTQ demographic data in health surveys in the future, but recognized the current reality.
“For now, we know that the virus doesn’t care about gender, but that having physical vulnerabilities, a high-risk job, no paid leave, smoking, lacking safe housing, or living in an institutional setting (such as a shelter, jail, or nursing home) all put you at greater risk,” Tobin said. “Trans people, on average, are more likely to experience each one of these risk factors.”
States and the CDC aren’t collecting data on whether COVID-19 patients identify as LGBTQ despite a recent joint letter declaring LGBTQ people would be vulnerable to the epidemic.
More than 150 advocates warned LGBTQ people would be disproportionately affected by the coronavirus because they smoke and suffer from cancer at higher rates; have high reported rates of discrimination in the health care system; and are disproportionately affected by HIV/AIDS.
(However, Dr. Susan Henn, chief medical officer for the D.C.-based Whitman-Walker Health, has told the Blade for people with well-managed HIV, the increased risk would only be “very slight.”)
The letter takes note ensuring “surveillance efforts capture sexual orientation and gender identity as part of routine demographics” would be a crucial goal to achieve in serving LGBTQ people during the COVID-19 epidemic.
Dr. Scott Nass, president of GLMA: Health Professionals Advancing LGBTQ Equality and a Palm Springs, Calif.-based family physician, said LGBTQ advocates will continue to beat the drum for LGBTQ inclusion in health surveys despite states declining to do that during the coronavirus crisis.
“GLMA has long advocated for data collection inclusive of sexual orientation and gender identity as central to ensuring the health and well-being of LGBTQ people,” Nass said. “Given the potential risk factors for LGBTQ individuals, inclusive data collection at federal and state levels may reveal important and life-saving data about the coronavirus and LGBTQ people and that’s exactly why GLMA, the National LGBTQ Cancer Network and more than 150 organizations called for data inclusion in our open letter on COVID-19 and LGBTQ communities.”
The Department of Health & Human Services added a question on sexual orientation to the National Health Interview Survey, the principal source of information on the health of the U.S. population. Although the administration was sluggish to add questions on transgender status, the Obama administration eventually allowed states to ask both sexual orientation and gender identity questions on the Behavioral Risk Factor Surveillance System, or BRFSS, if they so choose.
Scout said allowing states to include the LGBTQ questions on health surveys “has actually proven unexpectedly strong as political winds shifted” and now around 35 states made the inquiry on BRFSS, but “that’s still not full U.S. data.”
“Collecting SOGI data on electronic health records is rare as hens teeth,” Scout said. “This leaves us with all of our health issues masked for anything that is reliant on real time or end stage disease reporting (save HIV which has a separate system). Thus, in a time like today, we will only be able to measure which LGBTQ people had COVID years after the fact through self-report of people who have survived and happen to live in a state that collects SOGI on their BRFSS, and then only if BRFSS coordinators decide to add a COVID question.”
Amid concerns a lack of federal protections leaves LGBTQ people open to discrimination, a group of 87 House Democrats are calling on Dr. Deborah Birx to affirm anti-LGBTQ discrimination will be prohibited in coronavirus relief efforts.
The March 26 letter, coordinated by Rep. Deb Haaland (D-N.M.), Rep. Sharice Davids (D-Kansas) and the LGBTQ Equality Caucus, draws on the assertion LGBTQ people are disproportionately vulnerable to the coronavirus.
“We call on you to keep these considerations in mind as you develop solutions and we ask you to be proactive by publicly asserting that any programs or initiatives that assist the American people during this crisis must be conducted without discrimination against any community, including the LGBTQ community, and that there are no grounds by which this type of discrimination is acceptable,” the letter says.
LGBTQ people are disproportionately vulnerable to the coronavirus, the letter says, because that have high reported rates of discrimination in the health care system; have greater rates of smoking, cancer and depression; and are disproportionately affected by HIV/AIDS, which can depress immune systems and make patients vulnerable to disease.
Older people are vulnerable to the coronavirus, and LGBTQ elders even more so, the letter says, because they “grew up in an era where asserting an LGBTQ identity was difficult to impossible” and now have limited social support.
Birx, named the White House Coronavirus Response Coordinator, has become a rising star as result of her diplomatic approach to answering questions during the daily White House briefings on the pandemic.
As the House Democrats’ letter notes, Birx also has a history in fighting the HIV/AIDS epidemic. Since 2014, she has served as ambassador-at-large and U.S. Global AIDS Coordinator since 2014, which makes her responsible for the President’s Emergency Plan for AIDS Relief, or PEPFAR.
“Based on your many years of service in the fight against HIV/AIDS, we take comfort knowing that you are in this leadership position and have been, and will continue to be, an ally to the LGBTQ community,” the letter states.
Birx has compared the coronavirus pandemic to the fight against HIV/AIDS in the early days of the epidemic during a White House briefing in the Rose Garden earlier this month.
“We had another silent epidemic: HIV,” Birx said. “And I just want to recognize the HIV epidemic was solved by the community: the HIV advocates, and activists who stood up when no one was listening and got everyone’s attention. We’re asking that same sense of community to come together and stand up against this virus.”
House Democrats write the letter in the aftermath of the Trump administration declaring it will refuse to enforce an Obama-era rule barring anti-LGBTQ discrimination among federal grantees, such as taxpayer-funded adoption agencies and medical care providers. The Department of Health & Human Services had implemented the rule in December 2016 just before Obama left the White House and Trump took office.
Faced with calls to lift the rule from religious-affiliated non-profits, including Catholic Social Services, the Trump administration announced late last year it would not only the start the rule-making process to lift the regulation, but cease enforcing it immediately.
Earlier this month, a trio of LGBTQ legal advocacy groups filed a lawsuit against the decisionto stop enforcing the rule in court, citing the discrimination LGBTQ people may face in social services, such as meals on wheels, without the implementation of the rule.
Although House Democrats don’t explicitly mention the rule or the lawsuit, they cite many of the same concerns expressed in the lawsuit against the Trump administration.
“For every community impacted by coronavirus, you will often see ways in which the LGBTQ populations within those communities face harsh realities,” the letter says. “Young people whose colleges are closing may not have supportive families who will take them in. LGBTQ people who lose their jobs may have a harder time finding new work based on pre-existing patterns of discrimination against LGBTQ job-seekers. Those LGBTQ people in prison or who are navigating the immigration system already face unique challenges, including vulnerability to violence, which can be made worse during a crisis such as this.”
The record-setting $2 trillion deal Congress reached on Wednesday to stimulate the economy amid the devastation of the coronavirus pandemic contains $155 million to bolster HIV programs serving the nexus of communities affected by both diseases.
For the Ryan White HIV/AIDS Program, the deal includes $90 million for existing contracts under the law and the Public Health Service Act. At the same time, the deal appropriates $65 million for the Housing Opportunities for Persons with AIDS, or HOPWA, to maintain operations and provide rental assistance amid the coronavirus crisis.
In both cases, the money must be used by Sept. 30, 2022, although appropriations for HOPWA afford some additional flexibility. The money is on top of the $330 million Congress appropriated in December 2019 for Ryan White and other initiatives in fiscal year 2020 as part of the Trump administration’s initiative to beat HIV by 2030.
The money for the HIV programs is geared toward ensuring recipients — which include cities, states and community health centers — can continue and expand those services as the coronavirus pandemic complicates efforts to address HIV.
Rachel Klein, deputy executive director of the AIDS Institute, said the additional money for Ryan White programs, which provides care to low income people with HIV, is essential for HIV-positive people trying to obtain services amid the coronavirus pandemic.
“The program itself needs to be able to adapt to provide care in different ways,” Klein said. “People are trying to avoid sitting in public meeting rooms unnecessarily right because they don’t want to be exposing themselves potentially to a new virus. The programs are going to need to be able to be flexible, to find creative ways to ensure that people are able to still get the care that they need, and that’s going to come with some costs.”
There are mixed opinions about whether people with HIV are more at risk for COVID-19. On one hand, HIV if left untreated will depress a patient’s immune system and make them more susceptible to disease, but Dr. Susan Henn, chief medical officer for the D.C.-based Whitman-Walker Health, has told the Blade for people with well-managed HIV, the increased risk would only be “very slight.”
Lauren Killelea, director of public policy of the National AIDS Housing Coalition, said money for HOPWA is needed because people with HIV without access to housing “are less likely to be virally suppressed and therefore more susceptible to COVID-19.”
“HOPWA is uniquely situated to be a great, flexible resource for low-income people living with HIV during the coronavirus pandemic,” Killelea said. “HOPWA can not only provide permanent housing but also short-term assistance as well as critical supports like access to transportation and nutrition services.”
After failed votes in the U.S. Senate and negotiations throughout the week, congressional leaders had announced Wednesday morning they had reached a deal on Stage 3 for congressional action in response to the coronavirus crisis.
A vote was expected earlier Wednesday after the Senate returned from recess, but proceedings were halted over objections from a small cadre of Republicans — including Sens. Tim Scott (S.C.), Ben Sasse (Neb.) and Lindsey Graham (S.C.) — over language they say could lead to the exploitation of unemployment benefits. After leaders agreed to an amendment to appease these lawmakers, the Senate voted to approve the measure 96-0.
The next step is House approval for the stimulus package and President Trump signing the package into law, both of which were expected to happen expeditiously.
A number of parties had pressed Congress for the HIV funds in the stimulus package. Last week, AIDS United and a coalition of 90 HIV/AIDS and LGBTQ groups, including GLAAD, the Human Rights Campaign, Whitman-Walker Health, NMAC, NASTAD, NCSD and the AIDS Institute, sent a letter to every member of Congress urging them to consider people with HIV and “craft a relief package that takes the unique needs of this population into account.”
In a letter to Congress dated March 17 and obtained by the Blade, the White House Office of Management & Budget sought money in the stimulus package for Ryan White and other health programs to the tune of $1.336 billion. An attached request from Health Resources & Services Administration makes that request for “health centers to expand triage and treatment capacity and telehealth, rural hospital technical assistance and the Ryan White HIV/AIDS Program, in response to coronavirus.”
The request, however, makes no mention of HOPWA funds, which the Trump administration sought to cut earlier this month in its budget request for fiscal year 2021. OMB didn’t respond to the Blade’s request to comment on whether it welcomes the HIV money appropriated in the stimulus package.
Killelea said the HOPWA money was inserted by the Transportation and Housing & Urban Development Act appropriations staff headed by Sens. Susan Collins (R-Maine) and Jack Reed (D-R.I.) and Reps. David Price (D-N.C.) and Mario Diaz-Balart (R-Fla.). (Diaz-Balart was the first member of Congress confirmed to test positive for the coronavirus.)
Congress makes the appropriations at the same time the Trump administration has made a pledge to beat HIV in the United States with a PrEP-centric plan that aims at reducing new infections by 75 percent in five years and 90 percent by 2030.
Carl Schmid, executive director of the HIV & Hepatitis Policy Institute and co-chair of Presidential Advisory Council on HIV/AIDS, told the Blade the extra money is needed because the coronavirus threw a “monkey wrench” in the HIV plan.
“I was just talking today to someone at the CDC that several people from the center for that are working on HIV are being used to address COVID-19, and it’s a significant amount of their staff, because they all have the expertise in infectious diseases, and the doctors, too, in the field,” Schmid said. “That’s why I can see a lot of this 90 million being used to, for the doctors in the workforce.”
As Congress advances the deal, the Health Resources & Services Administration’s HIV/AIDS Bureau was set to have a phone conference with grant recipients and stakeholders across the country on Thursday at 3:30 p.m., according to a notice shared with the Washington Blade.
With the coronavirus claiming thousands of lives across the globe, medical experts are throwing any and all medications they can against the disease , including drugs used to treat HIV/AIDS that — if effective in clinic trials — may turn attention toward Truvada, commonly used as PrEP for HIV prevention.
One medical expert told the Washington Blade if the early promising results for the HIV drug Remdesivir hold out in clinical trials, the drug Truvada — the more standard medication against HIV/AIDS — could also work against the coronavirus.
David Hardy, adjunct professor of medicine for the Division of Infectious Diseases at Johns Hopkins University School of Medicine, said if Remdesivir works, Truvada could be shown to be effective because the two drugs are in the same family of medications.
“If Remdesivir works, because it falls into the same class of medication as Truvada, then Truvada may be able to be tried as well,” Hardy said.
Hardy said Remdesivir and Truvada — both developed by Gilead Sciences — work by the same “mechanism of action,” hitting the virus in a susceptible point in the virus’ replication cycle.
“I would wager to say that if the clinical studies that are studying Remdesivir in China and then in the U.S. now show some promise, then there’s gonna be a very quick look at Truvada to see if it works,” Hardy said.
Although Hardy said he’s unaware of any clinical trials underway for Truvada against coronavirus as of last week, he predicted that would change soon if Remdesivir is shown to be effective.
Hardy said there’s a key difference between the drugs: Truvada as a pill can be administrated orally, in contrast to Remdesivir, which requires intravenous injection.
“That can be much more complicated for treating large numbers of people than pills are,” Hardy said.
As reported by NBC News, there’s hope for Remdesivir, a drug used to fight HIV, which is still being studied under clinical trials. Based on early tests, the drug “may start working within 24 hours of the first dose” against the coronavirus.
According to anecdotal reports, at least two hospitalized patients who received Remdesivir started to improve by the next day. One was a man who traveled to Wuhan, China, where the virus originated, then after coming back to his home in Washington State became the first person in the United States diagnosed with COVID-19. And Chris Kane, 55, was diagnosed with the coronavirus and given the drug during his hospitalization at Providence Regional Medical Center in Everett, Wash.
In both cases, the patients started to improve after taking Remdesivir within one day.
But with this limited sample, questions remain about whether it was the drug that led to health improvement, or whether these two patients would have gotten better anyway.
The drug’s use against coronavirus is now officially in clinical trials at Providence Regional Medical Center and first results are expected in late April, according to NBC News. The hospital didn’t respond to the Blade’s request for comment and offered limited information to NBC News, citing an inability to discuss the drug before trials are complete.
As scrutiny on Remdesivir’s potential grows, Gilead Sciences announced on Monday in a statement it will eventually expand access to the drug, but — for the time being — suspend acquisition under early compassionate use.
“During this transition period, we are unable to accept new individual compassionate use requests due to an overwhelming demand over the last several days,” the statement says. “We are focused now on processing previously approved requests and anticipate the expanded access programs will initiate in a similar expected timeframe that any new requests for compassionate use would have been processed.”
Another exception Gilead Sciences set for compassionate use requests for Remdesivir was for pregnant women and youth under age 18 with confirmed COVID-19 infection and severe manifestations of the disease.
Remdesivir was among the drugs potentially effective against the coronavirus mentioned by President Trump, who touted the medication at a White House news conference last week.
Hardy warned despite reports HIV medication may be effective against the coronavirus, patients taking the drugs either for prevention or treatment may still be susceptible to COVID-19 and able to transmit it.
“People have misinterpreted when they have read this that HIV drugs work against the coronavirus that this means that they are somehow protected against the coronavirus by virtue of taking HIV drugs, and that is not something that anyone should assume at this point in time,” Hardy said. “We have no idea whether they work against the virus in any great numbers of people who have been taking the medications.”
The HIV drug Truvada is used not only for HIV treatment, but also prevention and in the form PrEP is seen as a key tool to ending the HIV epidemic. Asked by the Blade if HIV drugs are, in fact, proven to be effective in treating the coronavirus, that also would mean they would be effective in prevention, Hardy cautiously replied, “Maybe. Maybe.”
“There’s many, many factors that are involved when we study the same medication for two different infections,” Hardy said. “You know the dose of the medication that may work in HIV may not be enough. So, we don’t know whether or not the dose of medication that works for HIV is going to be the same.”
Medical experts across the board are cautious about raising hopes about potential medications against the coronavirus. For example, Trump’s public mention of drugs tested against the coronavirus without clinical determination they will be effective has inspired criticism from political opponents and from medical professionals.
After Trump tweeted out the unproven claim a combination of hydroxychloroquine and azithromycin has a “real chance” to fight the coronavirus, there were consequences. According to ProPublica, the tweet triggered a run on the medication, which is needed for individuals suffering from lupus, including an estimated 1.5 million Americans and several who reported not being able to obtain the medication.
Trump’s suggested use of unproven drugs against coronavirus led to a now infamous fiery exchange during a White House briefing between NBC News correspondent Peter Alexander, who asked whether it was giving people “false hope.” Trump then attacked Alexander in response to a subsequent question, and said he should be ashamed of himself.
Dr. Anthony Fauci, director of the National Institutes of Allergy & Infectious Diseases, pushed back against Trump’s untested claim hydroxychloroquine and azithromycin would be effective against coronavirus when asked about it Thursday during the White House Coronavirus Task Force briefing.
“I’m not entirely sure what the president was referring to, but believe it was a report of hydroxychloroquine and azythromicin,” Fauci said. “Many of the things you hear out there are anecdotal reports. They may be true – but the only way to know is randomized trials.”
Medications for several diseases are on the table for potential use against the coronavirus, including drugs used to treat malaria, such as chlorquine, which is considered one of the best hopes to fight the disease.
For another HIV drug, Kaletra, which is a combination of lopinavir and ritonavir produced by AbbVie, early tests indicated the drug would be effective, but that didn’t bare out in a major clinical trial.
Early indications Kaletra could be used against coronavirus were tested on an elderly couple from Italy, who were treated in India with the drug and whose test went from positive to negative, as well as a man in Spain.
The results on the couple tested in India were so promising that India’s Union Health Ministry had been recommending the treatment.
But hopes for Kaletra quickly faded, after a study released last week in the New England Journal of Medicine, according to Reuters.
A test in Chinese patients with severe coronavirus infection found the 99 who received Kaletra fared no better than the 100 who received standard care over the course of 28 days. All of the patients had pneumonia and were treated at Jin Yin-Tan Hospital in Wuhan, the city where the pandemic began.
According to Reuters, test participants who took Kaletra showed small improvements in their health, but “the differences were not statistically significant.” The drug was also shown to have side effects, prompting the treatments to be halted in 13.8 percent of patients.
Kaletra, however, was not tested against a placebo, which is considered the most effective way to assess a treatment.
Despite the lack of placebo and modest gains shown in patients taking Kaletra, Hardy said the trial results are dispositive.
“I do think that the verdict on Kaletra has been made…and it is negative,” Hardy said, “This study is rapidly being circulated in medical circles now.”
Regardless of the medication that ends up working, odds are likely the treatment for coronavirus will be available well before a vaccine.
Even with clinical trials underway now, health officials have said it would take between 12 to 18 months before a vaccine would be available to the public. In contrast, Hardy estimated a treatment for coronavirus for individuals who are infected would be ready within six to eight weeks.
Hardy said the effectiveness of treatment will ultimately be gauged on whether or not people infected with coronavirus and taking the medication are able to beat a death rate estimated one time at 3.8 percent.
“If that 3.8 percent can be reduced by giving people Remdesivir, then that will actually prove it works in terms of just giving them supportive care like a ventilator and things like that,” Hardy said.
Dr. Anthony Fauci, a leading voice of medical authority as the world confronts the coronavirus, is no stranger to viral epidemics — nor protesters who once displayed him in effigy in frustration amid new infections and rising death tolls.
At the height of the HIV/AIDS crisis in the early 1990s, Fauci was at the frontlines as director of the National Institutes of Allergy & Infectious Diseases, a role he began in 1984 and continues to this day. During that time, Fauci’s research contributed to the understanding of HIV’s destruction of the immune system and therapy that has significantly contained the disease in more recent years.
Now, as a member of the White House Coronavirus Task Force, Fauci has provided sage advice, calmed fears, and — at times — acted as voice of accountability for the Trump administration amid efforts to contain COVID-19.
As the coronavirus epidemic began to unfold, Fauci himself compared the situation to the early days of the HIV epidemic — as well as other diseases — because “there’s still a lot that’s unknown.“
“It’s not that different than the very early years of the HIV epidemic, of the anthrax attacks, of the concern about the pre-pandemic bird flu,” Fauci said March 9 on CNN’s “New Day.” “Everything has a little bit of a different twist to it. It’s not exactly the same, but there’s always that uncertainty that gets people very anxious.”
Under Fauci’s leadership, NIH in 1987 developed AZT, or zidovudine, the first antiretroviral approved for the treatment of HIV, although the epidemic continued. After more research, when combinations of drugs were seen to be effective against HIV, NIH cleared the way for more effective therapy in 1996.
Carl Schmid, executive director of the HIV & Hepatitis Policy Institute, was among the advocates fighting HIV/AIDS who hailed Fauci’s work both then and now.
“No one does a better job at explaining and conquering infectious diseases, whether it is HIV/AIDS or coronavirus, than Tony Fauci,” Schmid said. “Not only is he one of the world’s top infectious disease doctors but he knows how to articulate complicated issues and on top of it, understands how to address them utilizing an all parts of society approach. He has been there since the earliest days of the AIDS crisis and can take all of what he has learned and done over the years, including working with presidents of both parties, to now deal with the coronavirus.”
But it wasn’t always a happy relationship with HIV/AIDS activists. As the HIV/AIDS epidemic raged and continued to the claim the lives of thousands of gay men, Fauci was the target of activists who accused him of not moving quickly with new medicines to fight the disease.
According to the article, written by veteran Blade reporter Lou Chibbaro, Jr., more than 1,000 demonstrators marched through the sprawling grounds of the NIH “using placards, costumes, bull horns and red-colored tape to draw attention to their demand for faster government action on AIDS research programs.”
One photo taken at the event by the Blade — but never published until now — shows three protesters dressed in black robes and skull masks in the style of the Grim Reaper.
The three hold a large coffin-like box with letters reading, “Fauci: Resign Now — Release Compound: O.” Another holds a sign reading, “120,000 AIDS Deaths, Courtesy NIH.” Another holds up a pole within a bloody head mask on top and a sign underneath designating the effigy as “Fauci.”
“Scores of drugs and alternative treatments languish untested while more than 200 new cases of AIDS are diagnosed each day,” stated ACT UP in papers distributed at the demonstration.
Police reportedly arrested 61 protesters during the four-hour demonstration and charged them with trespassing, including five members of ACT UP/D.C.
Following the demonstration, Fauci reportedly said he was sympathetic to ACT UP’s cause, but believes its allegations were untrue. Further, Fauci was quoted as saying NIH implemented recent changes to direct more resources to fight infections diseases like HIV/AIDS.
ACT UP protest at the National Institutes of Health on April 21, 1990. (Washington Blade archive photo by Doug Hinckle)
A chief critic of Fauci was Larry Kramer, a longtime HIV/AIDS activist who helped found ACT UP in the late 1980s and remains hostile to this day. As recently as 2015, Kramer in an op-ed for The Advocate faulted Fauci for failing to live up to his promise to find a cure for HIV infection. (Kramer didn’t respond to a Blade email this week to comment on Fauci’s approach to the coronavirus.)
Kramer’s harsh words may be persiflage. Fauci was quoted in a 2012 article in the New Yorker about Larry Kramer as saying he’s come to regard the activist as a friend, crediting his work with instituting a major change in medicine against infectious diseases.
But to say the relationship between HIV/AIDS activists and Fauci was entirely frosty would be inaccurate. On Dec. 22, 1990, also as reported by the Blade, when President George H.W. Bush met with gay men with AIDS at NIH, Fauci was among those who took part in the discussion.
Also at the meeting was first lady Barbara Bush and George Bush, Jr., otherwise known as future President George W. Bush. It was the first time “a sitting U.S. president formally met with open gays,” the Blade reported at the time.
The presidential party, Fauci reportedly said, listened to the gay men in attendance and sat in on a support sessions for people undertaking NIH’s experimental AIDS drug trials. Some of the men had HIV, some had developed AIDS, the Blade reported.
The elder Bush shook hands with each of the men and presented them with a commemorative presidential tie pin, according to the Blade.
“He was really touched,” Fauci was quoted as saying. “This was not just a formality. He was really interested.”
The meeting, Fauci reportedly said, was open to the White House press corps and news photographers took photos of the elder Bush shaking hands with the men.
“But much to his disappointment, Fauci said, almost all the photos appearing in the nation’s daily newspapers the next day were of a different part of the NIH visit — when the president cradled babies with AIDS in the NIH pediatric ward,” the Blade reported.
Asia Russell, executive director of the New York-based group HealthGAP, was among the HIV/AIDS activists at the time and told the Blade this week that work was responsible for pushing Fauci into supporting the community.
“Dr. Fauci has been the target of AIDS activists’ campaigns and protests in the past, and those protests delivered results — they helped him see how access to the benefits of science is not neutral, it’s driven, or hindered, by politics, and that remains true today,” Russell said.
Thirty years after the massive protest at NIH, the nature of the virus inspiring fear among the public and responsible for the deaths of thousands worldwide has changed, but Fauci’s work has not.
Russell said Fauci in his role within the White House Coronavirus Task Force has brought to the fore shortcomings in the Trump administration’s approach to COVID-19, which she said “has been a disgrace.”
“It’s an embarrassment that Dr. Fauci, a trusted voice in public health, has to testify before Congress and make the rounds on the Sunday shows to contradict the lies the president is telling,” Russell said.
(Washington Blade photo by Chris Johnson)
In media appearances and testimony before Congress, Fauci has made clear the severity of the coronavirus. Meanwhile, President Trump has falsely said Americans are at “low risk” of contracting the disease, predicted “it will go quickly” and said testing was available to everyone.
“It is a failing. Let’s admit it,” Fauci said last week in the testimony before the House on the lag in testing availability. Days later, Trump declared under questioning in a Rose Garden press conference he would “not take responsibility” for the delay in tests, which weren’t delivered on a massive scale until last week.
When Trump said a vaccine for coronavirus would be ready in two months (which the White House retconned as a reference to an Ebola vaccine), Fauci told the reporters it would be more like 12 to 18 months even on an expedited basis.
Fauci has also given credit to Trump, who continues to tout his travel ban on China amid early reports about the coronavirus of the evidence of his prescience about the danger. Addressing reporters last week in a White House gaggle, Fauci said that move “absolutely” made a difference in limiting new infections in the United States.
Amid self-imposed quarantines, travel bans and recommendations people not meet in groups with more than 10 people, Fauci has also reassured the American public any perception the federal government is overreacting is misplaced.
“I’ll say it over and over again: When you’re dealing with an emerging infectious diseases outbreak, you are always behind where you think you are if you think that today reflects where you really are,” Fauci said. “That’s not word speak. It means: If you think you’re here, you’re really here, because you’re only getting the results; therefore, it will always seem that the best way to address it were to be doing something that looks like it might be an overreaction.”
Michael Ruppal, executive director of the AIDS Institute, said Fauci is a trusted voice because “his communication is straight forward and direct and isn’t convoluted by political spin.”
“Dr. Fauci has been a trailblazer and leader in the HIV/AIDS pandemic since the beginning,” Ruppal said. “He has been a trusted federal partner to the HIV/AIDS community, and we appreciate having him continue to lead efforts at NIH after all these years and advancements. Dr. Fauci has been thrust forward as the federal face of the U.S. response and his integrity and honesty speaks for itself throughout his handling of this uncharted and unprecedented territory regarding COVID-19.”
But Fauci isn’t the only member of the White House Coronavirus Task Force who cut their teeth on epidemiology during the time of the HIV/AIDS crisis.
Among them is Deborah Birx, U.S. Global AIDS Coordinator & U.S. Special Representative for Global Health Diplomacy at the State Department, whose three-decade-long career has focused on HIV/AIDS immunology, vaccine research and global health.
At a White House briefing on Monday, Birx recalled the fight against HIV/AIDS during the height of the epidemic, urging Americans to exhibit the same tenacity in the struggle against the coronavirus.
“We had another silent epidemic: HIV,” Birx said. “And I just want to recognize the HIV epidemic was solved by the community: the HIV advocates, and activists who stood up when no one was listening and got everyone’s attention. We’re asking that same sense of community to come together and stand up against this virus.”
Russell had favorable words for both Fauci and Birx in their approach to the coronavirus pandemic amid her general criticism of the Trump administration.
“The administration’s delays, dissembling, and political games are killing people,” Russell said. “Dr. Fauci and Ambassador Birx know that activists are watchdogging this effort and are ready to raise the alarm.”
Also on the White House Coronavirus Task Force with a history of HIV research is Robert Redfield, director of the Centers for Disease Control. In addition to his work against the coronavirus, Redfield is seen as the point-person for the Trump administration’s plan to beat HIV/AIDS in the Untied States by 2030.
In an interview last year with the Washington Blade, Redfield credited the LGBTQ community for coming forward to participate in testing during the early of the HIV/AIDS epidemic, saying that led to medical advances that helped thwart the disease.
But Redfield notably hasn’t been present at the White House briefings with the rest of the coronavirus task force. Meanwhile, media reports have indicated White House officials have blamed him for the sluggishness in the rollout of coronavirus testing capabilities.
White House Deputy Press Secretary Judd Deere rejected the notion Redfield’s absence was of any significance. “CDC is based in Atlanta, which is where Dr. Redfield is needed, and he’s actively involved in the work of the task force and stopping the spread of COVID-19,” Deere said.
An attendee at a fundraising dance party in Miami for the National LGBTQ Task Force has tested positive for the coronavirus, the organization informed participants last night in a letter shared with the Washington Blade.
The organization — best known for its annual “Creating Change” conference — informed attendees of the event Sunday night about the attendee who tested positive for coronavirus via a letter from Rea Carey, executive director of the National LGBTQ Task Force.
“I was informed that one of our Winter Party Festival guests tested positive for COVID-19 in the week following our event,” Carey said in a news statement Monday. “We are grateful to them for alerting us, particularly given that they were not experiencing symptoms during WPF and had traveled elsewhere, but wanted to make sure we were aware of this development.”
The Winter Party, which took place this year March 4 to 10, is a week-long celebration of beach parties and nightclub dancing in Miami. According to the Task Force, the official number of attendees at the event was 5,500 people.
It’s unknown how the attendee was infected. The Task Force as of Monday morning had yet to report other cases of attendees testing positive for coronavirus.
Carey said in the letter “there are many places people could have been exposed before and after Winter Party as this virus has developed.”
But coronavirus infection among event attendees doesn’t appear to be isolated to one individual, based on an account of one participant at the event.
The attendee, who spoke to the Blade on condition of anonymity, said Monday he had direct exposure to one friend who subsequently tested positive for the coronavirus.
“Within my group of friends, 10 or so of us have flu-like symptoms,” the attendee said. “I’ve chatted with acquaintances who in most cases say that they have many sick friends within their groups as well.”
The attendee added he’s part of a group chat with roughly 80 members and an estimated 20 of them say they have flu-like symptoms.
“Most of us are not eligible for testing so are self quarantined and recovering at home,” the attendee said.
Based on social media posts, the attendee said there could be up to three confirmed cases of Winter Party attendees who tested positive for coronavirus.
Carey insisted in a news statement the Winter Party was still held amid concerns about the spread of the coronavirus based on “official guidance available at the time.” Precuations undertaken at the event, Carey said, included comprehensive signage with CDC information about practicing good hygiene and making alcohol-based hand sanitizer available throughout the Festival.
“Information and circumstances have changed rapidly since WPF,” Carey said. “We continue to encourage all WPF guests to monitor their health, practice social distancing, wash hands with soap, use hand sanitizer and contact their doctor if they think they are exhibiting symptoms. If one tests positive for COVID-19, we urge them to contact those they were in direct contact with so all can take steps to monitor their health and speak with their doctors.”
The Washington Blade has placed a request for comment with the Task Force about whether there are additional reports of infections.
In the aftermath of the Winter Party, Miami Beach Mayor Dan Gelber said during a news conference Sunday the beach would be closing from 5th Street to 15th Street, and there would be an 11 p.m. curfew in the entertainment district, according to a local report from NBC Miami.
“We can’t have the kinds of crowds we’ve had, the kinds of gatherings,” Gelber was quoted as saying. “I walked down Ocean Drive yesterday and what I saw was incredibly disturbing, it wasn’t just the typical large gatherings of people, but it was young people who believe they’re invincible and probably don’t really think of this in any way as a health crisis.”
The Task Force’s decision to move forward with the Winter Party last week was met with anger on social media Monday in the aftermath of the report over coronavirus infections and warnings all public events should be cancelled.
With states still threatening to pass legislation aimed at restricting access to transition-related care for transgender youth, LGBTQ advocacy groups and major U.S. businesses are warning the enactment of such measures could have dire economic consequences.
The focus of the warning is an open letter, complied by the Human Rights Campaign and Freedom for All Americans, which was signed by 40 major business against anti-trans bills and made public Wednesday.
“Laws that would affect access to medical care for transgender people, parental rights, social and family services, student sports, or access to public facilities such as restrooms, unnecessarily and uncharitably single out already marginalized groups for additional disadvantage,” the letter says. “They seek to put the authority of state government behind discrimination and promote mistreatment of a targeted LBGTQ population.”
Among the 40 companies that signed the letter are Airbnb, Amazon, American Airlines, Apple, AT&T, Google, Hilton, IBM Corp,. Lyft, Marriott International, Microsoft, Nike, PayPal and Uber.
In numerous state legislatures, lawmakers have introduced bills aimed at restricting access to transition-related care, such as hormone therapy, puberty blockers and transgender surgeries, for youth below age 18. Other measures seek to inhibit transgender youths’ ability to play in school sports consistent with their gender identity.
One measure against transition-related care for youth in South Dakota was killed in committee, but others are still pending before legislatures and, in some cases, advancing forward.
In Alabama, the Senate approved this week SB219, which would not only ban transition-related care for youth, but require school officials and medical practitioners to out transgender youth to their parents. The House version of this legislation, HB303, has been approved in committee.
In Arizona, the House last month approved legislation, known as HB2706 and the “Save Women’s Sports Act,” seeking to block transgender youth’s participation in sports.
In the letter signed by 40 businesses, the companies make a veiled threat those companies may not bring money to states that pass legislation along these lines.
“As we make complex decisions about where to invest and grow, these issues can influence our decisions,” the letter says. “America’s business community has consistently communicated to lawmakers at every level that such laws have a negative effect on our employees, our customers, our competitiveness, and state and national economies.”
In a conference call with reporters on Wednesday, LGBTQ rights advocates said the potential economic costs of the anti-trans legislation is clear.
Carmarion Anderson, the Human Rights Campaign Alabama State Director, urged lawmakers to look at those potential costs when considering the legislation.
“These national corporations can see that anti-transgender grandstanding and demonization only hurts the state of Alabama, the entire LGBTQ community and their own bottom line,” Anderson said.
Anderson said organizers are engaged in conversations with lawmakers in Alabama, including Speaker Mac McCutcheon, to ensure the anti-legislation is defeated, and killed with inaction as the legislature session comes to an end. The last day of the regular session of the Alabama legislature is May 18.
The Washington Blade has placed a request in with McCutcheon seeking comment on his plans for the legislation.
Also on the call was Dan Eggers, an 18-year old transgender youth in Alabama who told his personal story about struggling with suicidal ideations and eating disorders before obtaining transition-related care.
“For the first time in my life, I’m healthy and genuinely happy,” Eggers said. “That is directly because of these treatments. In fact, after I received the treatments that I needed my middle school gym teacher, after spotting me from across the room, sought out my mother and told her he never seen me experience joy before that moment.”
The Alabama legislation, Eggers said, the measure would have “require[d] him to report my identity before I was ready, exposing me to higher risks of violence at home, and even homelessness.”
An estimated 30 percent of transgender people experience homelessness, Eggers said, and the average age of being kicked out is 13-and-a-half.
Bridget Sharpe, Arizona state director for the the Human Rights Campaign, echoed the sense businesses are fully behind efforts in Arizona to defeat anti-trans legislation.
“Major businesses understand that supporting equality isn’t only isn’t only the right thing to do, it’s good businesses sense,” Sharpe said. “Legislation promoting discrimination directly affects businesses: Full stop.”
The nationwide letter from the 40 businesses builds on a letter specific to the anti-trans legislation in Arizona signed by around 200 local and national businesses, including the Arizona State Tourism Association and the Arizona Diamondbacks.
Also on the call was Jennifer Brown, the mother of a transgender athlete, whose daughter — whom she referred to as “K” to protect her anonymity — competed on the men’s crew team in Fairfax, Va, before transitioning and joining the women’s team.
“There are many reasons that rolling on that women’s team was so incredibly important for K,” Brown said. “At a point in time when she hated almost every piece of her body, rowing was a gift that her body gave back to her. It gave her a reason to keep herself safe and healthy. Being part of a team, a team that depended on her, gave her a reason to go on.”
Brown said her daughter is now in college in Arizona may be found at the campus gym on the rowing machine.
According to data from Change Research presented by the Human Rights Campaign, 55 percent of Arizona residents, including 58 percent of Independents, believe supporters of the Arizona anti-trans bill are “further stigmatizing already vulnerable children to push their political agenda and further divide us.”
Further, the poll found 64 percent of Arizona residents believe the legislators are too focused on divisive issues and only 1 percent of Arizona Republicans say legislation on transgender issues should a top priority.
A Human Rights Campaign spokesperson said a similar poll wasn’t available in Alabama at this time.
Kasey Suffredini, CEO of Freedom for All Americans, said in a statement the letter from the 40 companies show the business community has “consistently taken a strong stand opposing legislation that discriminates against LGBTQ workers and customers.”
“Business leaders understand that discrimination is bad for business, and their economic competitiveness relies on fair and inclusive work and community environments for their employees and their families,” Suffredini said.
The sponsor of HB303 in the Alabama House, State Rep. Wes Allen, and the sponsor of SB219 in the Alabama Senate, State Sen. Shay Shelnutt, didn’t respond to the Blade’s request to comment on the economic threat to the state over the legislation.
Shelnutt, defending the legislation on the Alabama Senate floor, was quoted in AL.com as saying SB219 was necessary because kids should not be “given experimental drugs or surgeries that could have irreversible consequences for the rest of their life.”
“Kids are not fully developed until later in life,” Shelnutt reportedly said. “I think we can all agree that kids aren’t capable of making certain decisions until certain ages. And so, we want to just stop these procedures from happening in Alabama.”
The sponsor of HB2706 in Arizona, State Sen. Nancy Barto, couldn’t be reached for comment on the potential business impact of the bill.
“This bill is about fairness,” Barto told ABC News at the time it passed in the Arizona House. “That’s it. What is fair on the field, the court, the track and in the pool.”
The Alabama and Alabama chambers of commerce also didn’t respond to the Blade’s request to comment on the anti-trans legislation pending in their respective state legislatures.
LGBTQ rights advocates can point to precedent on anti-trans legislation having dire economic consequences.
After North Carolina enacted House Bill 2, which bars transgender people from using restrooms in state-owned buildings consistent with their gender identity, economic boycotts resulted in an a loss of more than 1,750 jobs and more than $77 million in investments and visitor spending, according to a 2016 analysis from Time Warner Cable News.
Cathryn Oakley, state legislative director for the Human Rights Campaign, said on the call she doesn’t have a specific dollar amount for potential economic costs to states that pass anti-trans legislation, but North Carolina is a good example.
“It’s not difficult to connect the dots between…exactly what happened in North Carolina and HB2 with businesses saying, ‘Look we’re not coming here,’ and these businesses speaking out at this point.” Oakley said.
As scrutiny of the treatment of transgender inmates continues to grow, the California prison system has updated its policy on transition-related care, including gender reassignment surgery, although the new guidance is getting mixed reviews at best from transgender advocates.
One transgender advocate said the document “appears to contain some important improvements,” but “there are still a few areas where the policy appears problematic or unclear.” Another said the changes “do nothing to change” access to transition-related care for inmates. In defense of the policy, a spokesperson for the California prison system says the new guidance is “expected to improve access to care.”
The California Department of Corrections & Rehabilitation, which is credited with being the first state prison system to implement any policy granting transgender inmates access to gender reassignment surgery, shared the updated 30-page guidance and a summary with the Blade last week.
The new guidelines, developed by California Correctional Health Care Services, dedicate a full page to specific criteria for granting inmates gender reassignment surgery: Persistent gender dysphoria; being at least 18 years old; having continuously used hormone therapy for 12 months; full-time living in a new gender role and keeping any other medical and mental health conditions well-controlled.
“Individuals may live successfully as transgender persons without surgery,” the guidelines say. “Gender affirming surgery may be considered for those individuals who are diagnosed with Gender Dysphoria and demonstrate significant distress not attributable to conditions of confinement, mental illness or other factors, but are due to lack of reasonable response to available nonsurgical treatments and there are no available, additional treatments other than surgery that are likely to improve or alleviate their symptoms.”
In a letter dated Nov. 8, 2019 to the Blade, the state prison health system reveals 130 inmates requested male-to-female gender reassignment surgery since the policy was announced, but only seven were granted the procedure in the same time period. Meanwhile, 51 inmates requested female-to-male gender reassignment surgery, but only 10 obtained the procedure.
Terry Thornton, a California Department of Corrections spokesperson, told the Blade this week the new policy came out, however, because guidelines “are continually revised to align with community standards and as needed to ensure operational efficiency.”
The California prison system isn’t done. Thornton said a supplement to the transgender inmate guide on requests for gender reassignment surgery is currently undergoing a revision, but it’s unknown when that will be complete.
The previous policy, established in 2015, was brokered by then-California Attorney General Kamala Harris as a result of lawsuits filed by transgender inmates Michelle Lael-Norsworthy, who was serving time for second-degree murder, and Shiloh Quine, who’s serving a life sentence for first-degree murder, kidnapping and robbery. Both inmates had obtained medical clearance for gender reassignment surgery and sought the procedure, but were denied.
(In response to the Blade report last year that few inmates were granted gender reassignment surgery despite the deal Harris brokered — and promoted on the campaign trail — the California Democrat’s presidential campaign said the the policy should be reviewed because anti-transgender bias may be in play. Harris’s Senate office didn’t respond to the Blade’s request to comment on the update.)
Ensuring transgender prisoners have access to gender reassignment surgery, which would come at taxpayer expense, has been a controversial issue and may even soon be adjudicated by the U.S. Supreme Court as a result of a case percolating up from Idaho.
But the key difference in the new California policy seems to be hormone therapy, not gender reassignment surgery.
Thornton said the new guidance provides guidelines on hormone therapy for transgender inmates to primary care doctors as opposed to endocrinology specialists, which she said “is expected to improve access to care.”
“The new Transgender Care Guide, which more clearly aligns with WPATH criteria, expands its education to primary care providers and gives a more detailed step-by-step approach to care for transgender men and transgender women,” Thornton said. “This new guide improves education for providers about the terminology and diagnoses related to transgender care.”
Thornton added the guidance updates access to hygiene items and clothing for transgender inmates.
“All of these improvements will enable primary care providers the ability to more effectively meet the needs of the transgender population,” Thornton said. “CCHCS and CDCR will continue to expand education to providers and patients about transgender care.”
Despite the changes, advocates for ensuring transgender inmates have access to gender reassignment surgery were largely unimpressed, saying the guidelines still hamper access to transgender-related care.
Shawn Meerkamper, senior staff attorney with the San Francisco-based Transgender Law Center, flat-out rejected the changes.
“For years, California’s prisons have had in place a sham policy that serves to deny critical and often life-saving health care to the overwhelming majority of trans people who need it,” Meerkamper said. “Unfortunately, these updates do nothing to change that reality for the hundreds of transgender people in California prisons who desperately need access to medically necessary transition-related surgeries.”
Harper Jean Tobin, director of policy at the National Center for Transgender Equality, took a more nuanced approach, saying the new guidance “appears to contain some important improvements,” but at the same time “there are still a few areas where the policy appears problematic or unclear.”
For starters, Tobin took issue with the California prison system housing transgender inmates consistent with their gender identity in sex-based facilities on a case-by-case basis as opposed to implementing a blanket policy ensuring a mismatch won’t happen.
“The new policy says prisoners ‘have traditionally’ been housed based on external genitalia, and ‘may possibly be moved’ following surgery,” Tobin said. “CDCR also says that new state legislation ‘may allow’ placement consistent with gender identity in other cases — but in fact that is already permitted and under federal law it is required to be considered in every case.”
A recent NBC News report from Kate Sosin documents the conditions transgender inmates face across the United States, few are housed consistent with their gender identity, and that mismatch can have dire consequences.
Of the 10 transgender women at a Chino, Calif., facility who spoke to NBC News during a weekend visit last year, nine reported having been sexually assaulted behind bars. Half said they’d sought a transfer to a women’s prison, but were denied.
Other issues transgender inmates face, per the NBC News report, include not being called by the name they prefer.
Tobin also criticized the guidance’s incorporation of self-injurious or suicidal behaviors as factors that could prevent a transgender inmate from obtaining treatment for gender dysphoria, which she said “appears contrary to the standards of care.”
“Nearly 40 percent of transgender adults have attempted suicide at some point, suicidal ideation is even more common, and ‘self-injurious behaviors’ could include attempts at self-surgery among patients facing denials or prolonged delays in care,” Tobin said. “These may be severe symptoms of GD, not contraindications to treatment, and CRDC’s policy should not suggest otherwise without great caution.”
Further, Tobin faulted the guidelines for calling on medical providers to rule out other mental health disorders in inmates that may co-occur or mimic gender dysphoria before providing transition-related care, saying that practice is contrary to standards from the American Psychological Association and the World Professional Association for Transgender Health.
“Accepted clinical guidelines for gender dysphoria recognize that co-occurring mental health conditions are common, because gender dysphoria itself can cause depression and anxiety, and because being transgender makes individuals a target for abuse and trauma,” Tobin said.
Thornton, in response to concerns about housing in the updated guidelines, said placement for all inmates, not just transgender inmates, takes many factors into account.
“All inmate housing is evaluated on a case-by-case basis, which includes an inmate’s criminal history, behavior, rehabilitation opportunities, medical and psychiatric needs, program needs as well as their safety and security,” Thornton said.
As an example, Thornton said a transgender man requesting a hysterectomy would not be moved to a male facility following the procedure, while a transgender woman undergoing a vaginoplasty would be moved.
With respect to ruling out other mental health conditions being a requirement before treating gender dysphoria, Thornton said that practice is consistent with medical standards as defined by the World Professional Association for Transgender Health.
“People who engage in self-injurious or suicidal behaviors may have other mental health concerns that, until optimally managed, could possibly preclude medical treatment of gender dysphoria,” Thornton said.
All in all, Thornton said, the updated guidelines demonstrate a commitment from the California prison system to provide adequate treatment and facilities for transgender inmates.
“CDCR is the only prison system routinely approving gender-affirming surgery and is working to build trust with its patients, their families, and community advocates,” Thornton said. “CDCR has policies in place to improve safety, help prevent sexual abuse, create a more respectful environment, improve outcomes for reentry and improve medical care for its incarcerated transgender community and is committed to creating safe and humane environments for all people housed in California prisons.”