The first at-home cervical screening device is currently under clinical trial to become FDA-approved in the USA, and we think it’s about time for a change.
For women and those with uteruses, undergoing a regular pap smear to prevent cervical cancer can be an unpleasant experience thanks to the speculum used.
The outdated device used in pelvic appointments to separate the vaginal walls can be cold and uncomfortable. The clamp-like instrument was invented in the mid-19th century and hasn’t adapted much since its origins.
The new device called Teal Wand, designed by women-led company Teal Health, is an at-home cervical cancer screening device. The brand explained in an Instagram post that the at-home screening device “follows the American Cancer Society’s cervical cancer guidelines and runs the samples on approved primary HPV assays”.
Teal Health’s initial study of the device revealed that 97% of women said the at-home cervical cancer screening device was easy or very easy to use. Meanwhile, 92% of participants said they would choose self-collect over the current standard of care with a clinician collecting, while 87% said they would be more likely to get screened if the Teal Wand was an option.
In the US, the Centres for Disease Control and Prevention estimates that around 4,000 women and people with uteruses die of cervical cancer a year. Self-collected cervical screening tests are already an option in other countries and actively reduce the barrier for women and LGBTQ+ people facing healthcare-based discrimination.
The Australian Government introduced such tests in July 2022. The home kit tests “allow privacy and help break down barriers for thousands of people who have never screened – including women who have experienced sexual violence, LGBTQIA+ people and culturally and linguistically diverse and First Nations communities”, the Department of Health and Aged Care website reads.
“Australia has always punched above its weight when it comes to cervical cancer, and now Australia is on track to be the first country in the world to eliminate this deadly disease,” said the assistant minister for the department The Hon Ged Kearney.
Unsurprisingly, the original device has bleak origins. In 1945, Dr James Marion Sims performed surgeries on enslaved women without anaesthesia or pain relief, in a bid to understand the reproductive system. He invented the instrument to allow himself – and largely Cis male doctors – the ability to better look at the vagina and cervix, GE HealthCare explains.
The U.S. syphilis epidemic isn’t abating, with the rate of infectious cases rising 9% in 2022, according to a new federal government report on sexually transmitted diseases in adults.
But there’s some unexpected good news: The rate of new gonorrhea cases fell for the first time in a decade.
It’s not clear why syphilis rose 9% while gonorrhea dropped 9%, officials at the U.S. Centers for Disease Control and Prevention said, adding that it’s too soon to know whether a new downward trend is emerging for the latter.
They are most focused on syphilis, which is less common than gonorrhea or chlamydia but considered more dangerous. Total cases surpassed 207,000 in 2022, the highest count in the United States since 1950, according to data released Tuesday.
And while it continues to have a disproportionate impact on gay and bisexual men, it is expanding in heterosexual men and women, and increasingly affecting newborns, too, CDC officials said.
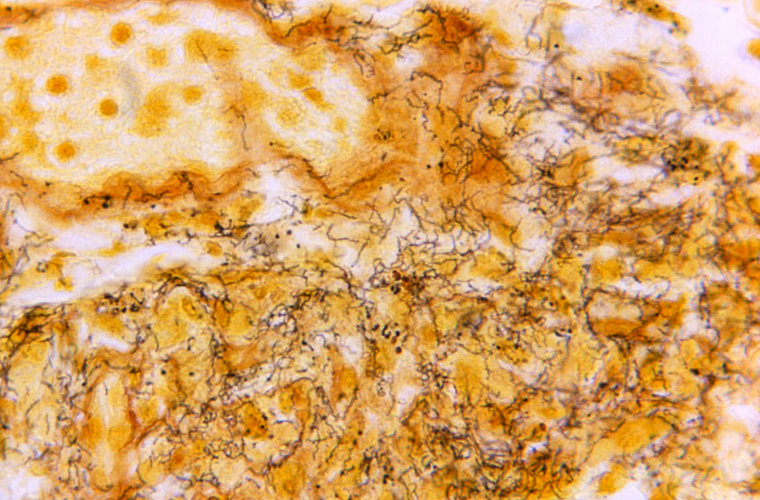
A tissue sample with the presence of the bacterium responsible for causing syphilis.Skip Van Orden / CDC via AP file
Syphilis is a bacterial disease that can surface as painless genital sores but can ultimately lead to paralysis, hearing loss, dementia and even death if left untreated.
New syphilis infections plummeted in the U.S. starting in the 1940s when antibiotics became widely available and fell to their lowest by 1998.
About 59,000 of the 2022 cases involved the most infectious forms of syphilis. Of those, about a quarter were women and nearly a quarter were heterosexual men.
“I think its unknowingly being spread in the cisgender heterosexual population because we really aren’t testing for it. We really aren’t looking for it” in that population, said Dr. Philip Chan, who teaches at Brown University and is chief medical officer of Open Door Health, a health center for gay, lesbian and transgender patients in Providence, Rhode Island.
The report also shows rates of the most infectious types of syphilis rose not just across the country but also across different racial and ethnic groups, with American Indian and Alaska Native people having the highest rate. South Dakota outpaced any other state for the highest rate of infectious syphilis at 84 cases per 100,000 people — more than twice as high as the state with the second-highest rate, New Mexico.
South Dakota’s increase was driven by an outbreak in the Native American community, said Dr. Meghan O’Connell, chief public health officer at the Great Plains Tribal Leaders’ Health Board based in Rapid City, South Dakota. Nearly all of the cases were in heterosexual people, and O’Connell said that STD testing and treatment was already limited in isolated tribal communities and only got worse during the pandemic.
The U.S. Department of Health and Human Services last year convened a syphilis task force focused on stopping the spread of the STD, with an emphasis on places with the highest syphilis rates — South Dakota, 12 other states and the District of Columbia.
The report also looked at the more common STDs of chlamydia and gonorrhea.
Chlamydia cases were relatively flat from 2021 to 2022, staying at a rate of about 495 per 100,000, though there were declines noted in men and especially women in their early 20s. For gonorrhea, the most pronounced decline was seen in women in their early 20s as well.
Experts say they’re not sure why gonorrhea rates declined. It happened in about 40 states, so whatever explains the decrease appears to have occurred across most of the country. STD testing was disrupted during the COVID-19 pandemic, and officials believe that’s the reason the chlamydia rate fell in 2020.
It’s possible that testing and diagnoses were still shaking out in 2022, said Dr. Jonathan Mermin, director of the CDC’s National Center for HIV, Viral Hepatitis, STD and TB Prevention.
“We are encouraged by the magnitude of the decline,” Mermin said, though the gonorrhea rate is still higher now than it was pre-pandemic. “We need to examine what happened, and whether it’s going to continue to happen.”
Large numbers of queer young people of colour in the US believe they have a low life expectancy compared with their white peers, a new study has found.
The research for LGBTQ+ youth mental-health charity The Trevor Projectshowed that, overall, 58 per cent of young queer people believe there is a high chance they will live to at least the age of 35, while 34 per cent view their chances as low. The remaining respondents were unsure.
The report, which surveyed 28,524 LGBTQ+ people between the ages of 13 and 24, found that 59 per cent of young LGBTQ+ people of colour think they will live to 35 and beyond, while 69 per cent of their white peers think there is a high chance they will live to the same age.
That disparity was even greater for transgender and non-binary people (53 per cent), compared with cisgender people, with 79 per cent of those surveyed believing they would live at least that long.
Steven Hobaica, a research scientist at The Trevor Project, told Advocate that as well as factors such as supportive parents and access to gender-affirming care, people who expressed high levels of “life purpose” were more likely to expect to live longer.
“We found that white LGBTQ+ young people were more likely to endorse a higher chance of living past 35 compared [with] their peers of colour, possibly due to generally having less stressful life experiences,” Hobaica said.
“It is well documented that youth who hold multiple marginalised identities, such as LGBTQ+ youth of colour, report higher rates of both stressful life events and mental health problems than their white LGBTQ+ peers, which may help explain these findings.”
‘Change is needed’
In addition, the research showed that queer people who believed they had a lower life expectancy were also more likely to have had recent bouts of anxiety(82 per cent) and depression (77 per cent).
This group also reported higher rates of self-harm in the past 12 months (77 per cent), suicide consideration (69 per cent), and suicide attempts (28 per cent) compared with respondents who thought they would lie longer (41 per cent, 24 per cent, and six per cent, respectively).
These latest figures in particular led The Trevor Project to highlight the need for investment in LGBTQ+ mental health care.
“Systemic policy change is needed to address the mental health of LGBTQ+ youth,” Hobaica said.
Several factors compounded this, with Black trans and non-binary youth experiencing higher levels of depression, anxiety, homelessness and discrimination.
“Simply put, the mental health of Black transgender and non-binary young people is a public-health crisis,” Dr Myeshia Price, a senior director of research science at The Trevor Project, said at the time.
Suicide is preventable. Readers who are affected by the issues raised in this story are encouraged to contact Samaritans on 116 123 (www.samaritans.org), or Mind on 0300 123 3393 (www.mind.org.uk). Readers in the US are encouraged to contact theNational Suicide Prevention Line on 1-800-273-8255.
Gender dysphoria diagnoses in the United States increased in all but one state in recent years, suggesting that a growing number of transgender people are seeking health care.
Gender dysphoria “refers to psychological distress that results from an incongruence between one’s sex assigned at birth and one’s gender identity,” according to the American Psychiatric Association.
Not all transgender people experience dysphoria. Treatment can include social shifts, such as wearing different clothing or going by a different name, or medical affirmation, which can involve puberty blockers, hormone treatment, and surgery. Medical treatment — gender-affirming care — typically requires a diagnosis from a health care professional before patients can receive it.
Despite a growing number of states seeking to ban gender-affirming care for minors and restrict the care for adults, more people are beginning to seek it by receiving a diagnosis, a recent report from Definitive Healthcare found.
Virginia, Indiana, and Utah were the states with the greatest increase in diagnoses between 2018 and 2022 The only state to see a decrease was South Dakota, which banned gender-affirming care for minors in 2023.
South Dakota lawmakers had attempted to pass legislation banning care in 2020, which the report stated likely had “the dual chilling effects of reduced access to sympathetic providers and the self-directed seeking of care in states where long-term access was protected.”
The report also noted that “other states with bans on gender-affirming care for youth have seen year-to-year dips in gender dysphoria diagnoses, too,” though this does not necessarily indicate that less transgender residents are seeking care, but rather “possibly indicating that shifting social and political climates have pushed young patients and their parents to seek diagnoses in states that are friendlier to trans people.”
For patients under the age of 18, gender dysphoria diagnoses increased from 17.5 percent to 20.4 percent during the four-year period. The report notes this could be reflective of transgender identities becoming “more accepted by society,” in spite of the legislators pushing health care bans.
The Williams Institute estimates that 1.6 million people in the U.S. are transgender, nearly 20 percent of them being between the ages of 13 and 17. Among transgender youth, 35.1 percent (105,200 total) live in states that have restricted access to gender-affirming care, according to the Human Rights Campaign.
Out Massachusetts Gov. Maura Healey (D) has proposed legislation to grant LGBTQ+ military veterans coverage for in-vitro fertilization (IVF), something the federal Veterans Administration (VA) only allows for heterosexual couples.
Healey first introduced the legislation – dubbed the HERO Act – in November, and according toThe Boston Business Journal a hearing on the proposal is set to be held this month before the Joint Committee on Veteran and Federal Affairs.
Related:
“Our veterans have sacrificed so much for our country, and this transformative legislation marks an important step toward ensuring that Massachusetts supports them in return,” Healey said in a press release after introducing the legislation.
Calling the bill “historic,” she added, “From day one, our administration has been committed to revitalizing veterans’ services in Massachusetts and ensuring that every one of these heroes receives the benefits, resources, and support that they deserve.”
The bill would no doubt have a massive impact, as veterans in same-sex marriages have made it clear the current policies affect them deeply. In August, Massachusetts veteran Ashley Sheffield filed a class action lawsuit against the VA arguing that the denial of fertility coverage to LGBTQ+ couples is unconstitutional.
“We are entitled to equal treatment and we should no longer be treated as second-class citizens,” Sheffield reportedly said when she filed the suit.
In addition to granting IVF coverage to same-sex couples, the HERO Act proposes a myriad of other benefits, including expanded access to mental health care treatment, an increase in the tax credits small businesses receive for hiring low-income and chronically unemployed veterans, an increase in flexibility for veteran property tax exemptions, and an expanded definition of a veteran dependent.
In November 2022, Healey became the first out lesbian governor in the country, as well as the first woman elected governor in her state. Before that, she was the country’s first out lesbian state attorney general.
As AG, she championed non-discrimination protections for trans people in Massachusetts and pushed for gender-neutral markers both federally and for the state. And as civil rights chief in the AG’s office, Healey brought the first successful challenge to the Defense of Marriage Act, helping to lay the groundwork for marriage equality nationwide.
After she won the Democratic primary, she stood before a raucous crowd of supporters and told them, “I am so proud to be able to stand before you tonight as your Democratic nominee for governor of Massachusetts.” She nodded to the sound of her latest title and added, “That sounds good.”
The former professional basketball player and captain of her team at Harvard describes herself as a “baller” and was clear-eyed about the work ahead in her remarks that night: “I ask you, as a former point guard, to leave it all with me on the court.”
Four days of waiting under the flickering fluorescent lights of UNC Hospitals’ emergency room left Callum Bradford desperate for an answer to one key question.
The transgender teen from Chapel Hill needed mental health care after overdosing on prescription drugs. He was about to be transferred to another hospital because the UNC system was short on beds.
With knots in his stomach, he asked, “Will I be placed in a girls’ unit?”
Yes, he would.
The answer provoked one of the worst anxiety attacks he had ever experienced. Sobbing into the hospital phone, he informed his parents, who fought for days to reverse the decision they warned would cause their already vulnerable son greater harm.
Although they initially succeeded in blocking the transfer, the family had few remaining options when a second overdose landed Callum back in UNC’s emergency room a few months later. When the 17-year-old learned he was again scheduled to be sent to an inpatient ward inconsistent with his gender identity, he told doctors his urge to hurt himself was becoming uncontrollable, according to hospital records given by the family to The Associated Press.
“I had an immense amount of regret that I had even come to that hospital, because I knew that I wasn’t going to get the treatment that I needed,” Callum said. “That moment of crisis and shock and fear, I would wish anything that that hadn’t happened, because I truly think that I took a step backwards from where I was before in terms of my mental health.”
As the political debate over health care for transgender youth has intensified across the U.S., elected officials and advocates who favor withholding gender-affirming medical procedures for minors have often said parents are not acting in their children’s best interest when they seek such treatment.
Major medical associations say the treatments are safe and warn of grave mental health consequences for children forced to wait until adulthood to access puberty-blocking drugs, hormones and, in rare cases, surgeries.
Youth and young adults ages 10–24 account for about 15% of all suicides, and research shows LGBTQ+ high school students have higher rates of attempted suicide than their peers, according to the Centers for Disease Control and Prevention.
Some transgender teens say the negative rhetoric popularized by many Republican politicians in recent years has become too much to bear. In North Carolina, legislators enacted new limits to gender-affirming care for trans youth this year while barely discussing flaws in the psychiatric care system. It’s one of at least 22 states that have passed laws restricting or banning gender-affirming medical care for transgender minors. Most face legal challenges.
North Carolina lacks uniform treatment standards across hospitals and runs low on money and staff with proper training to treat transgender kids in crisis. That means the last-resort measures to support patients like Callum often fail to help them, and sometimes make things worse.
Sending a transgender child to a unit that does not align with their gender identity should be out of the question, no matter a hospital’s constraints, said Dr. Jack Turban, director of the gender psychiatry program at the University of California, San Francisco, and a researcher of quality care barriers for trans youth in inpatient facilities.
“If you don’t validate the trans identity from day one, their mental health’s going to get worse,” Turban said. “Potentially, you’re sending them out at a higher suicide risk than they came in.”
When North Carolina lawmakers allocated $835 million to shore up mental health infrastructure earlier this year, none of the money was specifically allocated to the treatment needs of trans patients. Though the funding may benefit everyone, a lack of direct action has left trans youth at the mercy of a system ill-equipped to help them when they need it most.
Callum Bradford, center, and his team, carry their boat to the ramp as they get ready for a rowing club practice at Jordan Lake, in Apex, N.C., on Oct. 6, 2023. Erik Verduzco / AP
A nationwide dearth of pediatric psychiatric beds was compounded by the COVID-19 pandemic, which saw an unprecedented number of people seeking emergency mental health services, according to a report by the American Psychiatric Association. Demand has yet to return to pre-pandemic levels.
A “dire shortage” of at least 400 inpatient psychiatric beds for North Carolina youth has left UNC with no choice but to send patients to other facilities, even those that cannot accommodate specific needs, said Dr. Samantha Meltzer-Brody, chair of the UNC Department of Psychiatry.
Emergency rooms are not designed for boarding, nor can they provide comprehensive mental health treatment. That creates an immediate need to place patients left waiting in the ER for days or even weeks before a bed opens up, Meltzer-Brody said.
While UNC’s own inpatient program assigns all children to individual rooms on co-ed floors, it sends overflow patients to some hospitals that don’t make such accommodations.
“We have no choice but to refer people to the next available bed,” Meltzer-Brody said of the University of North Carolina-affiliated hospital. “If you’re talking about the LGBTQ+ community and seeking trans care, you may be sent to a place that is not providing care in a way that is going to be most optimal.”
Callum exploded when he was told about plans to place him in a unit for girls, his records note. He shouted and cried hysterically until he ended up in an isolation room. Doctors later found him banging his head against the wall in a trance-like state.
“It was almost as if sort of my brain had turned off because of such a shock,” he recalled. “I had never acted on such severe self-harm without even realizing that I was doing it.”
UNC declined to comment on Callum’s case, despite the family’s willingness to waive its privacy rights. But Meltzer-Brody did broadly address barriers to gender-affirming treatment for all psychiatric patients.
The public hospital system’s policy on gender-designated facilities recommends inpatient assignments based on a patient’s “self-identified gender when feasible.” But with the ER overrun in recent years, Meltzer-Brody said meeting that goal is a challenge.
The issue extends beyond transgender youth, affecting patients with autism, addiction and acute psychiatric disorders who are sometimes sent to facilities unfit to provide specialized care.
It doesn’t help, she said, that there is no national standard for how psychiatric hospitals must cater to transgender patients.
The LGBTQ+ civil rights organization Lambda Legal has outlined best practices for hospitals treating transgender patients under the Affordable Care Act. The organization says denying someone access to a gender-affirming room assignment is identity-based discrimination, based on its interpretation of the law.
But such cases rarely end up in court, because the burden falls on families to advocate for their rights while supporting a child in crisis, said Casey Pick, law and policy director at The Trevor Project, a nonprofit focused on LGBTQ+ suicide prevention.
“These are circumstances that are themselves often inherently traumatic, and adding a layer of trauma on top of that in the form of discrimination based on an individual’s gender identity just compounds the issue,” Pick said. “The last thing we should have to do is then add the additional trauma of going to court.”
Dan Bradford, left, and his son Callum, at their home in Chapel Hill, N.C., on Sept. 14, 2023. Erik Verduzco / AP
Parents including Callum’s father, Dan Bradford, describe feeling helpless while their children are receiving psychiatric care involuntarily, which isn’t uncommon after attempted suicide. Callum’s involuntary commitment designation also temporarily stripped his mother and father of many parental rights to make medical decisions for their son.
A psychiatrist himself, Dan Bradford always has supported his son’s medical transition, which began with puberty-blocking drugs, followed by a low dose of testosterone that he still takes. Eventually, Callum underwent top surgery to remove his breasts. Irreversible procedures like surgery are rarely performed on minors, and only when doctors determine it’s necessary.
“In Callum’s case, the gender dysphoria was so strong that not pursuing gender-affirming medical treatments, like pretty quickly, was going to be life-threatening,” his father said, wiping tears from his eyes. “Any risk that might be associated with the treatments seemed trivial, quite frankly, because we were afraid we’re going to lose our kid if we didn’t.”
North Carolina law bars medical professionals from providing hormones, puberty blockers and gender-transition surgeries to anyone under 18. But some kids like Callum, who began treatment before an August cut-off date, can continue if their doctors deem it medically necessary.
Although he retained access to hormones, Callum said it has been brutal seeing the General Assembly block his transgender friends from receiving the treatments he credits as life-saving.
“When these public policies are discussed or passed, that sends a really strong message to these kids that their government, their society and their community either accepts them and validates them or doesn’t,” said Turban, the researcher at UC San Francisco.
His research has found that many medical providers still lack training about LGBTQ+ identities and make common mistakes, such as printing the wrong gender designation on a hospital wristband or placing a transgender patient in a single-occupancy room when everyone else has a roommate.
Fearing the plan to place his son in a girls’ ward would be deeply traumatizing, Dan Bradford secured a spot at a residential treatment center in Georgia. He pleaded with UNC to release Callum early and convinced the North Carolina hospital that was supposed to take him to reject the transfer.
The teen then spent 17 weeks in an individualized treatment program in Atlanta, recovering from the circumstances that landed him in the ER and the added trauma he endured there. He has since returned home and is taking care of his mental health by playing keyboard and rowing with his co-ed team on the calm waters of Jordan Lake. For the first time in years, Callum said he’s thinking about his future.
There are some positive developments on the horizon for North Carolina youth facing mental health crises.
The new state funding for mental health services approved in October has enabled UNC Hospitals to open a 54-bed youth behavioral health facility in Butner, 28 miles (45 kilometers) north of Raleigh. State Department of Health and Human Services Secretary Kody Kinsley said the facility should alleviate some barriers to individualized care, including for transgender patients. And UNC has announced plans to open a freestanding children’s hospital within the next decade.
Leaders of the Butner facility, which began its phased opening this month, have promised to take a whole-family approach so parents are not shut out of their child’s treatment plan. Nearly every patient will be placed in an individual room on a co-ed floor.
The new facility and funding will allow more patients to stay in single-occupancy rooms at UNC, but overflow patients may still be sent elsewhere, Meltzer-Brody said. The hospital system has not changed its policies on transgender patient referrals, and other facilities across the state that receive those patients still lack uniform standards for treating them.
Although Callum said his experiences eroded his trust in the state’s inpatient care network, he is optimistic that the new resources could give others a more gender-affirming treatment experience, if they are paired with policy changes.
“I’m still here, and I’m happy to be here,” he said. “That’s all I want for all my trans friends.”
When talking about myths of people with disabilities, Katherine Allen says there’s more to deafness and blindness than people think.
“Just about everything [is on] a spectrum,” said Allen, who is visually impaired.
Allen, 68, is active in the Philadelphia-area disability and LGBTQ+ communities. She is an accessibility consultant for Philly Touch Tours, an organization that provides “equal opportunities in cultural settings for people with vision loss,” as per the organization’s website.
In collaboration with Trish Maunder, creative director and co-founder of Philly Touch Tours, Allen trains the staff of local museums and cultural institutions how to welcome people with disabilities as visitors to their establishments.
“This is a kind of sensibility, busting myths,” Allen said. “The hands-on training [is rooted in the question] ‘how would you guide or help a blind person? What’s the proper way to do that?’”
Allen and her colleagues often begin the conversation or title a presentation for these training sessions with the line, “It’s OK to say ‘nice to see you’ to a blind person.”
“People are afraid and blindness is one of the disabilities that really kind of freaks people out,” Allen said. “It makes them uncomfortable. They don’t know what to do or say.”
On the flip side, all of the blind people that Allen knows, especially those who use a cane, have been “accosted by well-meaning people that won’t take no for an answer,” she said. When people on the street ask a blind person if they need help, they just grab their arm without waiting for them to respond.
Debunking these misconceptions and missteps is part of the work that Allen does through Philly Touch Tours. She also facilitates activities and tours to help people who are blind or vision-impaired experience Philadelphia in an engaging way.
“We have a multisensory tour through the Italian market and we visit a group of vendors that are really open and friendly and cool with our people,” Allen said. “We work with a couple of the Ben Franklin [impersonators] doing history tours.”
Philly Touch Tours occasionally brings groups of people who are visually impaired to visit Philadelphia’s Magic Gardens, a space with an outdoor mosaic sculpture garden, rotating exhibits, and an exterior that’s laden with mosaic art.
“What’s so great about having Katherine on the team is that she herself has a disability. She has low vision,” Maunder said. “When we’re talking about training or we’re talking about making things accessible for people who are blind or [have] low vision, when she speaks, it’s a completely authentic voice. Mine is too because I have a daughter who’s 37, who’s blind.”
Separate from Philly Touch Tours, Allen and Maunder organize a monthly meetup group for blind and visually impaired people in Philly, the majority of whom are 50 and above. The group gets together to go to the beach, visit a local cathedral or simply go out to dinner. Allen and Maunder organize an annual holiday party for the group, which Allen will host for the second time in the community room at John C. Anderson Apartments (JCAA), where she lives. JCAA is an LGBTQ+-affirming apartment building in Philly for queer and trans people who are 62 and older.
Hosting the holiday party at JCAA “is especially nice because, especially [for] people that are blind, transportation access is really tough,” Allen said. “This is a Center City location. It’s a building that’s well-lit. It’s in-and-out.”
When Allen moved into JCAA, she met people from all walks of life, said her friend Eileen Plato, who owned the popular gay spot Judy’s Cafe in Philly, which opened in 1974 and has since closed.
“[Katherine] had a whole new community of folks with disabilities, without disabilities, [people who are] older, and multicolored and multi gender,” Plato said. “Anderson has all kinds of folks – straight, gay, trans.”
Allen’s work in the disability community is vital “because not that many people are involved,” Plato added. “It’s hard for somebody who has sight to plug into a community that doesn’t. Katherine’s able to get in there and make things happen, whether it’s taking people somewhere that they’ve never ever been and can’t imagine how they could get there, or going to a party with 30 blind people.”
“Katherine’s able to get in there and make things happen, whether it’s taking people somewhere that they’ve never ever been and can’t imagine how they could get there, or going to a party with 30 blind people.”Eileen Plato
none
When Allen isn’t working at Philly Touch Tours, organizing outings for the meetup group for the blind and visually impaired, or working in the garden at JCAA, she’s listening to a book on tape, reading The New York Times or the magazine published by AARP.
“[Katherine] doesn’t sit still,” Plato said.
AARP is the largest nonprofit in the U.S. that advocates for and empowers people who are 50 and older as they age.
Allen lost a significant part of her eyesight due to a macular incident in her 30s, she said. Nonetheless, she continued on as the art director for a magazine at Nielsen Publishing at the time. She was not immediately open about her low vision.
“[Katherine] will often talk about how it took her longer to come out as a low-vision person than it did to come out as gay,” Maunder said. “In that way, she makes sure it’s part of our framing and that immediately levels the playing field for everybody. She’s very warm. She’s very welcoming.”
In terms of how her vision impairment intersects with her identity as a lesbian, Allen said that blindness is her superpower.
“Because we don’t make visual judgments,” she said. “I can see, so I say ‘we,’ but especially [with] blindness, it puts you at a different point of view. You’re judged by the character you keep. [Having low vision] just gives me a better view.”
Over the last six years, blood center employee Dylan Smith was often asked how frequently he gave blood himself. His answer was always the same: As a gay man, he couldn’t.
That changed this month.
Thanks to new federal guidelines finalized in May, gay and bisexual men in monogamous relationships can now donate at many blood centers around the country without abstaining from sex.
Bloodworks Northwest, where Smith works as a donor services supervisor, adopted the change on Dec. 6. He and his partner gave blood for the first time the next day.
“It’s been really emotionally difficult just to explain every single time the reason why,” said Smith, 28. “To be able to finally step up and support the mission that I really have just believed in since I started here just makes my heart feel so happy.”
The new U.S. Food and Drug Administration guidelines are the latest step in a yearslong effort to reverse restrictions that were designed to protect the blood supply from HIV, but which were increasingly criticized as discriminatory following scientific advances that allowed better detection of the virus.
In 2015, the FDA dropped the lifetime ban on donations from men who have sex with men and replaced it with a one-year abstinence requirement. The agency shortened the abstinence period to three months in 2020 after donations plummeted during the COVID-19 pandemic.
The American Red Cross, which accounts for about 40% of blood and blood component donations in the U.S., began implementing the new guidance in August.
Posey, whose own life was saved by a transfusion when he fell down a set of stairs and broken glass sliced an artery, welcomed the new guidance, saying hospitals and patients need access to a new pool of donors. Manuel Valdes / AP
About half of the 16 independent blood bank organizations that are members of the Alliance for Community Transfusion Services have rolled out the new guidelines, with more expected next year, the organization said.
“It is going to take time,” said Benjamin Prijatel, president of Shepeard Community Blood Center in Augusta, Georgia. “Blood centers and health professionals are going to have to put forth the effort to engage and educate this community in order to overcome years of distrust. That’s the only way this rule change will translate into additional donations.”
The change puts the emphasis on sexual activity rather than on sexual orientation. All potential donors are screened with a new questionnaire evaluating their HIV risk based on sexual behavior, partners and other factors that can contribute to the spread of blood-borne infections, such as intravenous drug use or recent tattoos or piercings.
Potential donors who report having anal sex with new partners in the last three months are barred from giving until a later date, and anyone who has ever tested positive for HIV will continue to be ineligible. Those taking pills to prevent HIV through sexual contact are still barred until three months after their last dose; the medications, known as PrEP, can delay the detection of the virus, the FDA said.
Donated blood is then tested for HIV, hepatitis C, syphilis and other infectious diseases.
Bloodworks Northwest, which supplies blood to more than 90 hospitals in the region, isn’t keeping track of how many newly eligible donors are coming in, said Dr. Kirsten Alcorn, the nonprofit’s co-chief medical officer. But workers have heard plenty of stories from people excited to give.
“It feels very meaningful to many of them to now be able to contribute to somebody’s survival,” Alcorn said.
Bloodworks executive Aaron Posey, whose own life was saved by a transfusion when he fell down a set of stairs and broken glass sliced an artery, welcomed the new guidance. He said hospitals and patients need access to a new pool of donors.
“Having always witnessed a shortage in the blood supply, it has at times been very frustrating,” said Posey, who first donated blood during the pandemic when the abstinence period was cut to three months.
Smith learned of the restrictions on gay men giving blood when he was screened while trying to donate his freshman year of college in 2013. The rules blindsided him, he said. It was a long time to wait before he could finally donate with his partner and other friends.
“Just being able to see them donating next to me, smiling next to me … meant so much,” Smith said.
When marginalized groups face discrimination in the health care system, the results can be far-reaching and drastic. Across LGBTQ+ communities, this experience is all too well known. For years, activists have pointed out that health care for LGBTQ+ Americans is “under attack,” and bias is thriving. People frequently face gaps in health services, treatment, and outcomes.
There’s another aspect of this problem that needs to be addressed. It’s one that has a direct, immediate impact on the health and wellness of millions of people: an information gap. In many cases, LGBTQ+ Americans have learned not to trust traditional sources of health information. Many also have had trouble receiving the information they need from these sources when they ask for it. As a studyfound, “There is breadth of evidence documenting LGBTQ+ individuals’ experiences of heterosexism, homophobia, overt discrimination and pathologization in the health care setting, which has proven to be a barrier for LGBTQ+ individuals seeking health information from doctors.”
This problem doesn’t just apply to doctor’s offices. It also applies to other entities such as government health agencies, hospitals and pharmaceutical companies. We explored this in our new survey.
We found that LGBTQ+ Americans are substantially more likely to get sick due to a lack of information. Twenty-seven percent of LGBTQ+ respondents told us that they have gotten sick in the last 12 to 18 months because they did not have the information they needed to make decisions about their health. (Eighteen percent of non-LGBTQ+ respondents said the same.)
To be clear, LGBTQ+ Americans are active in seeking out health information. But the sources they’re turning to don’t always have all the accurate, relevant, inclusive information that they need.
We looked at where LGBTQ+ Americans are going when they need health information. Much like Black Americans, LGBTQ+ Americans have curated sources they trust. We call these “chosen circles.” Two findings in particular were striking.
Forty-one percent of LGBTQ+ respondents in our survey said they get health information from TikTok — a figure about twice as high as the 21% of non-LGBTQ+ respondents who said the same.
News reports have discussed the role of TikTok in reaching members of LGBTQ+ communities, particularly younger people. The San Francisco Chronicle podcast Fifth & Mission called the social media platform “a lifeline for LGBTQ youth.” Mashable reported that, according to the Trevor Project, TikTok is where LGBTQ+ youth of color feel safest and most comfortable online.
The fact that LGBTQ+ communities are specifically seeking health information on TikTok presents an opportunity for health agencies and organizations. They should build up their efforts on this platform. It’s up to them to make sure that videos are available, providing accurate, helpful information about a wide range of health topics.
They should also work with popular influencers on the platform to reach LGBTQ+ Americans with important health information. More than a third (36%) of LGBTQ+ respondents in our survey said that online influencers they follow are an important source of health information. And they share information as well. More than a third said they have shared their own health information, or reposted health information from other sources, on social media. So these platforms can be especially helpful in improving health outcomes.
In our survey, more than a quarter (28%) of LGBTQ+ respondents said they turn to mental health therapists and counselors for emotional support in making health decisions. Again, this figure is lower among non-LGBTQ+ Americans.
This offers another opportunity for health-focused agencies and organizations. By working with people who provide therapy and counseling to LGBTQ+ communities and getting them the latest, most useful information on all sorts of health problems, these agencies and organizations can reach people in need.
Our survey also finds that no matter where they’re getting information, LGBTQ+ Americans understandably want to see people like them front and center. They want information specifically designed to reach them, addressing their experiences and unique challenges. And in all communications, they want health information providers to show that they understand the broad diversity of LGBTQ+ communities, spanning different races, religions, gender identities and more.
The need for change is urgent. By listening to, learning from, and partnering with members of LGBTQ+ communities, health agencies and organizations can create real transformation, empowering people with information to live healthier lives.
Tayla Mahmud is the executive vice president of health equity and multicultural strategy with M Booth Healthm a health consultancy and communications agency. Peter Matheson Gay is its chief impact officer.
There are still hundreds of conversion therapy practitioners in the U.S., despite many state and local laws limiting the discredited and harmful practice of trying to change a person’s sexual orientation or gender identity.
A Trevor Project report released Tuesday, “It’s Still Happening,” identified more than 1,320 conversion therapy practitioners in 48 states and the District of Columbia. More than 20 states, D.C., and numerous cities and counties have enacted laws barring licensed professionals from subjecting minors to such therapy, but those laws don’t affect what counselors offer adult clients, nor do they affect the work of unlicensed practitioners, including many of those who are affiliated with a religious institution. Some faith-based therapists, however, do hold state licenses.
Many of the therapists the Trevor Project identified operate in states that have restrictions, according to the report. And the number is likely an undercount, given that “conversion therapy is increasingly underground and conducted in secret, with many practitioners not publicly advertising their services in a way that can be documented,” the document states.
“While public awareness of the harm and unscientific foundation of conversion therapy has grown dramatically over the years, many believe it to be a thing of the past. This new report shatters this misperception, revealing troubling evidence that conversion therapy is far from being a relic of history,” Casey Pick, director of law and policy for the Trevor Project, said in a press release.“Conversion therapy practitioners are widespread across the country, with many of them utilizing their licenses and credentials to attempt to legitimize the dangerous and unethical practices they aim to impose on vulnerable LGBTQ+ youth. The findings of this report underscore the urgent need for policymakers, state licensing boards, professional associations, accreditation agencies, healthcare leaders, and faith communities to take action today to end this insidious and exploitative industry.”
The Trevor Project’s researchers identified “more than 600 practitioners who hold active professional licenses and over 700 practitioners who operate in a ministerial (official religious) capacity,” the report says. They performed online searches and reviewed all leads that they uncovered.
Pennsylvania, Texas, Minnesota, Missouri, and Ohio had the most identified licensed and unlicensed practitioners, in descending order. Minnesota is the only state in this group with a ban on conversion therapy for minors. The South had the largest proportion of the providers identified — 33 percent — followed by the Midwest, with 28 percent. Hawaii and Vermont were the only states with no identified practitioners.
Conversion therapy has been condemned as ineffective and harmful by every major medical and mental health group in the U.S. The American Psychological Association has found it is “associated with an extensive list of long-lasting social and emotional consequences,” the report notes. “These include depression, anxiety, suicidality, substance abuse, a range of post-traumatic responses, loss of connection to community, damaged familial relationships, self-blame, guilt, and shame.”
It is rooted in the idea that being lesbian, gay, bisexual, transgender, or queer is a mental illness that needs to be “cured” — again, something rejected by leaders of the mental health field.
To end conversion therapy, Trevor Project officials call for more state laws limiting the practice and better enforcement of those that exist. They also urge the federal government to take action through regulatory bodies and for Congress to pass legislation classifying conversion therapy as consumer fraud — such legislation has been introduced but has yet to pass.
“Lifting the curtain and exposing this underground practice is a shocking realization of how much work still needs to be done to put a stop to the deeply entrenched conversion ‘therapy’ industry,” Troy Stevenson, director of state advocacy campaigns for the Trevor Project, said. “Governors and state lawmakers have a particularly unique responsibility to act — and act urgently. They have extraordinary power by way of legislation, regulation and executive action to end this abusive and pervasive practice across the country.”
“Every parent wants their child to be well and to thrive, which is what makes this report so astonishing, and frankly, frightening,” added Brian K. Bond, CEO of PFLAG National, a partner with the Trevor Project in the movement to end conversion therapy since 2012. “When therapists, counselors and trusted faith leaders misrepresent their services, families pay the price. Until lawmakers take action to end these practices, PFLAG National advises LGBTQ+ people and families to avoid services that promote therapies using terms such as ‘conversion,’ ‘reparative,’ ‘reintegrative,’ ‘unwanted same-sex attraction,’ ‘sexual attraction fluidity exploration,’ and ‘rapid-onset gender dysphoria.’’’