Gilead Sciences, the drug giant behind the blockbuster HIV prevention pill Truvada, won FDA approval on Thursday to market Descovy — a medication already used by those who have HIV — as its next-generation prevention drug.
Descovy is not yet approved for certain groups, including women who have vaginal sex, since its efficacy has not been studied in this population; for these patients, Truvada is an approved option.
“Descovy for PrEP provides a new HIV prevention option that matches Truvada’s high efficacy with statistically significant improvements in renal and bone safety, which can be an important consideration as people at risk increasingly use PrEP for longer periods of time,” Daniel O’Day, Gilead’s CEO, said in a statement.
Like Truvada, Descovy is taken once daily and can reduce the transmission of HIV by over 95 percent. According to GoodRx, a one month’s supply of Descovy and Truvada both retail for roughly $1,800, though few U.S. patients pay this price as PrEP is covered by private and public insurance.
Gilead has long been buffeted by HIV activists like the PrEP4All coalition over the high price of Truvada and the circumstances of Truvada’s development and testing, which was largely funded by private donors and the U.S. government. That information was first publicized by the Global Health Justice Partnership at Yale University, which wrote “based on our preliminary review, CDC’s Patents for PrEP appear to be valid and enforceable.”
Fewer minority men who are at risk for HIV take a prevention pill or discuss it with their doctors, U.S. researchers say.
Awareness of a pill for “preexposure prophylaxis,” or PrEP, is high for all groups of men who have sex with men. But lower proportions of black and Hispanic men, compared with white men, have actually gotten prescriptions for the drug, which is 99 percent effective at preventing HIV transmission, the study team found.
Based on interviews, researchers found the disparities emerge at the point of having a discussion about PrEP with a healthcare provider. This suggests doctors can do more to help close this gap, they write in the Centers for Disease Control and Prevention’s (CDC) Morbidity and Mortality Weekly Report.
“This type of research is critical to finding – and correcting – missed opportunities to offer PrEP to people at risk for HIV, particularly among African American and Latino gay and bisexual men,” said study leader Dafna Kanny of the CDC’s Division of HIV/AIDS Prevention.
National Gay Men’s HIV/AIDS Awareness Day is September 27. The “Ending the HIV Epidemic” national initiative aims to reduce new infections by 75 percent in five years and by 90 percent in 10 years.
“It’s important for providers to take sexual histories of gay and bisexual men and to discuss PrEP as an option for HIV prevention with those who could potentially benefit from it,” Kanny told Reuters Health by email. “These discussions also help to destigmatize PrEP use, which is particularly important for increasing PrEP use among African American and bisexual men.”
Kanny’s team analyzed interviews with more than 4,000 men who participated in the 2017 National HIV Behavioral Surveillance survey to understand who is using PrEP and why some are not using it.
Candidates for PrEP use include men with multiple male sex partners in the past year, a male sex partner with an HIV infection during the past year, condomless anal sex or a bacterial sexually-transmitted infection within the past year.
Overall, 95 percent of the white men in the study said they were aware of PrEP, along with 87 percent of Hispanic men and 86 percent of black men. Yet only 58 percent of whites, 44 percent of Hispanics and 43 percent of blacks said they discussed PrEP with a clinician in the past year.
About 42 percent of white men, 30 percent of Hispanic men and 26 percent of black men reported taking PrEP in the past year.
Among the steps from awareness to getting onto PrEP, discussing it with a healthcare provider seemed pivotal. Men who got that far were more likely to be using PrEP. Still, disparities remained. Among the 2,000 men who discussed PrEP with a clinician, 68 percent of white men reported PrEP use, compared with 62 percent of Hispanic men and 55 percent of black men.
These differences were not explained by a lack of insurance or a usual source of health care – typical barriers to accessing prescription medications.
Geographically, disparities in PrEP use were seen between white and black men in the South and West, and between white and Hispanic men in the South.
The CDC estimates that less than 25 percent of the more than 1 million Americans who could benefit from PrEP are using it, Kanny said. She added, “There is a critical need to address racial and ethnic disparities.”
Future studies will need to investigate other barriers to PrEP use, such as high deductibles and high co-pays, which affect racial and ethnic minorities in particular, said Brandon Marshall of the Brown University School of Public Health in Providence, Rhode Island, who wasn’t involved in the CDC study.
“If we continue to see these disparities, HIV infections will likely continue to grow,” he told Reuters Health by phone. “Our goals to end the epidemic will be out of our grasp.”
Recent research indicates that some doctors don’t prescribe PrEP because they believe it will lead to risky sexual behavior, Marshall noted, which may disproportionately affect racial and ethnic minority men.
“These race-based stereotypes held by some providers also continue to perpetuate mistrust of the medical community in racial/ethnic minority communities,” he said. “If you feel your healthcare provider isn’t listening to you or not addressing your needs, it’s time to find a different provider who has more experience with PrEP and can answer your questions.”
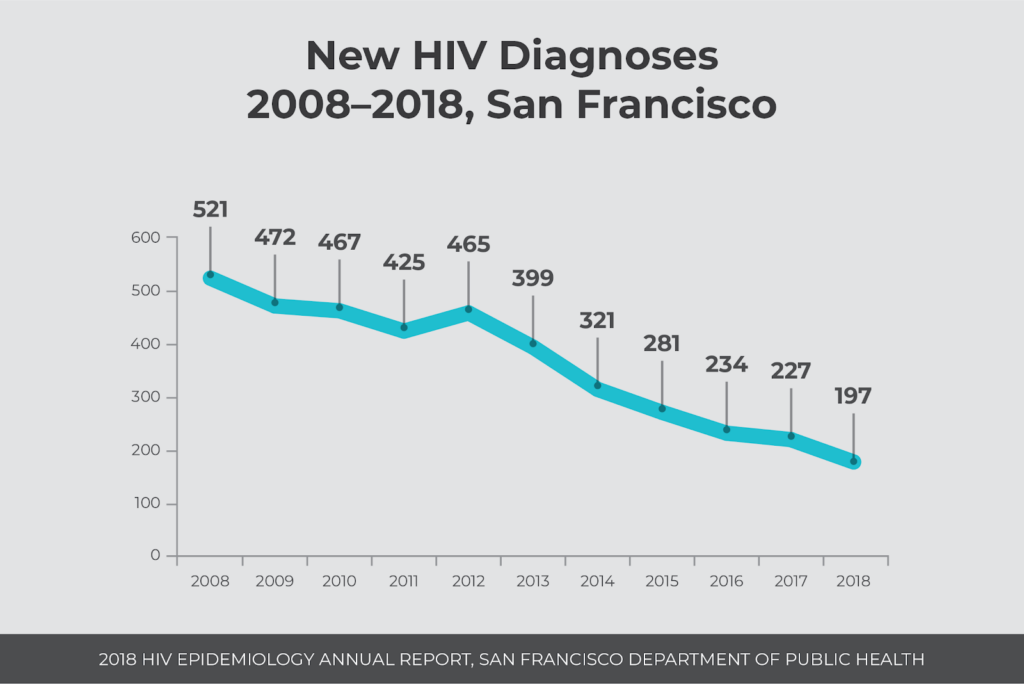
Every year, the San Francisco Department of Public Health (SFDPH) publishes a comprehensive report on HIV incidence and prevalence in the city, showing HIV trends to guide the public health response. Continuing a downward trend since the peak of the HIV epidemic in the 1990s, the most recent report with 2018 data shares a historic milestone reached by the city: Fewer than 200 HIV diagnoses occurred in San Francisco.
A total of 197 people were diagnosed with HIV last year in San Francisco. This is a 13% decline from 227 diagnoses made in 2017, and a 62% decline from 523 infections ten years ago in 2008. The peak number of HIV diagnoses in San Francisco occurred in 1992 with 2,327 diagnoses.
Most people (94%) living with HIV are aware of their status, and 91% of people newly diagnosed with HIV in 2018 entered care within one month. It is estimated that 74% of people with a last known address in San Francisco who are living with HIV were virally suppressed in 2017.
“I am really delighted that we in San Francisco, since the 1980s, have been at the forefront of pushing for innovative ways to change policies, new sciences and technologies to help us get to this milestone,” said Mayor London Breed at a press conference at Zuckerberg San Francisco General’s Ward 86. “This shows that when we work together with the community, with our policy makers, with our public health experts, and our nonprofits we can make a difference and save people’s lives.”
“We are pleased, but not satisfied,” said Diane Havlir, MD, who spoke on behalf of the Getting to Zero consortium. “We’re not satisfied because we had nearly 200 new diagnoses of HIV in our city—and it’s a preventable disease.”
Differences by Race and Ethnicity, Housing Status and for People who Inject Drugs
People of color, people experiencing homelessness and people who inject drugs continue to experience higher diagnosis rates, lower viral suppression rates and lower survival rates.
People of color are disproportionately affected by HIV
African American and Latinx men had the highest diagnosis rates (145 and 89 per 100,000), and rates increased from previous years. Diagnosis rates for white men have declined steadily since 2012. Among women, African Americans had a much higher diagnosis rate (35 per 100,000) than women of other races.
Overall, 74% of people living with HIV in San Francisco were virally suppressed, while viral suppression rates were lower for African Americans (68%), trans women (68%), women (66%), people who use injection drugs (65%), men who have sex with men who inject drugs (68%) and trans women who inject drugs (64%).
“San Francisco continues to make unprecedented progress towards ending the HIV epidemic,” said Joe Hollendoner, CEO of San Francisco AIDS Foundation. “However, we continue to see racial disparities related to HIV health outcomes. To end HIV transmission and AIDS-related deaths, the public health system needs to address the systemic racism that is inhibiting our progress.”
“We have to double down on these gaps that we’re seeing,” said Havlir. “We need to listen, and we need to deploy new innovative approaches with tools that have. With PrEP. And with upcoming tools like long-acting injectable [HIV] therapies which could make it a lot easier for some of our populations.”
Homelessness compounds HIV risk and severity of health outcomes
As the number of new HIV diagnoses shrinks year after year in San Francisco, and the number of people experiencing homelessness grows, a higher proportion of HIV diagnoses are occurring among people without access to medical care, social support and prevention resources—in particular people without housing.
In 2018, 20% (40) of new HIV diagnoses were among people without housing compared to 10% (29) in 2015. There were 8,011 people experiencing homelessness in San Francisco in January 2019, according to the 2019 San Francisco Homeless Point-in-Time Count and Survey, a 14% increase since 2013.
People without housing are also much less likely to be virally suppressed. Only 33% of people experiencing homelessness were virally suppressed, compared to 74% of people overall.
“We know that many elements that are key to success, for people living with HIV, are challenging if you don’t have a place to live,” said Monica Ghandi, MD, MPH, medical director of the SFGH HIV clinic. “That would be like making and keeping appointments. Where you store your medications, and where you keep them safe. Maintaining safe sex, and healthy eating. All of these barriers to taking your medications every day are amplified 100-fold if you don’t have a home.”
“Our focus on disparities really has to focus on ensuring that we reach people where they are,” said Hyman Scott, MD, MPH from Bridge HIV at SFDPH. “There are no ‘hard to reach’ populations—there are just ‘hard to deliver’ services. We need to re-think the way we approach some of these services that we deliver.”
HIV and people who inject drugs
People who inject drugs account for 25% of new HIV diagnoses, (10% are men who have sex with men who inject drugs; 1% are trans women who inject drugs; 14% are other people who inject drugs), a proportion which has risen over the years.
In addition to accounting for a higher proportion of HIV diagnoses, injection drug use is associated with worse health outcomes: People who inject drugs are less likely to be virally suppressed and have lower three-year survival rates after an AIDS diagnosis.
The percentage of people who are diagnosed with HIV who inject drugs is rising steadily every year, while reductions are seen in other populations including men who have sex with men.
“San Francisco has a robust syringe access program, which has kept HIV transmission rates low among people who inject drugs, but it’s not sufficient to eliminate HIV transmission among people who inject,” said Laura Thomas, director of harm reduction policy at San Francisco AIDS Foundation. “Housing instability and displacement make it challenging for people who use substances to always do so safely. That’s why it’s so important for us to establish safe injection sites in our city.”
“Unless we invest in expanding low barrier substance use and mental health counseling services like those offered at our Harm Reduction Center and at the Stonewall Project, I worry that increased HIV infection trends like those we’re seeing with people who inject drugs will continue,” said Mike Discepola, MA, senior director of behavioral health services and the Stonewall Project at San Francisco AIDS Foundation. “We will not get to zero new infections in San Francisco unless we focus services on our most vulnerable populations. This includes those who inject and use drugs, are experiencing homelessness or have untreated mental health concerns.”
An Aging HIV Population
With nearly 16,000 people living with HIV in San Francisco, two-thirds (10,691 people) are age 50 and older.
“We know that this is the generation that didn’t plan to live,” said Vince Crisostomo, manager of theElizabeth Taylor 50-Plus Network at San Francisco AIDS Foundation. “They didn’t plan financially, they didn’t set up 401Ks. But, they did live. And service providers need to be thinking about how to adjust services to meet the needs of these long-term survivors. How can we provide culturally competent services for people of older age who are living with HIV?”
“To end the epidemic we cannot leave anyone behind,” said Hollendoner. “We must achieve this ambitious goal together and prove to the world that it can be done.”
Guided by a new 5-year strategic plan, San Francisco AIDS Foundation charts a course for improving the sexual health outcomes of people of color and other priority communities, establishing safe injection sites, creating a comprehensive network of health and wellness services for people over age 50 who are living with HIV, and living our values of racial justice.
Over the years, HIV has evolved into a chronic condition necessitating life-long medication. Now, researchers are studying the efficacy and acceptability of long-acting HIV medications that may keep thevirus under control for a month or longer. Can long-acting therapies provide an alternative to daily dosing? And, what do people who stand to benefit from this way of dosing think about the possibility of not having to take daily oral medications?
“HIV has been part of my life for 33 or 34 years, and medication for almost 20,” said Efrén Solanas, a long-term survivor in the Bay Area. “I’ve been taking pills for so long, that routine is completely integrated into my life. Wherever I go, I take my pills. But not having to get prescriptions filled, worry about copays, or remember when I’ve taken my pills would definitely be an attractive option. It would be amazing to not have to worry about those things.”
Long-acting medications may be especially helpful for people who struggle with the routine of a daily pill.
“It’s not difficult to take daily medications, but it is inconvenient,” said Guillermo Velez, a San Franciscan who seroconverted in 1995 and started taking antiretrovirals in 1996. “Sometimes I just forget. By the fifth day of the week, sometimes I think, ‘Did I take my medication yesterday?’ Instead of dosing again, I just skip a day.”
Over more than 20 years of taking antiretrovirals, Velez has experienced horrendous side effects, complicated regimens and inconvenient dosing. “It’s always a trade-off,” he said. “These medications made us miserable, but they kept us alive. Over the years, meds have gotten better. To think that a new medication is effective, and also delivered once a month by injection—that would be such a convenience. You wouldn’t need to worry about keeping the medication stocked, or filling those medication trays.”
At the IAS 2019 conference in July, Miranda Murray presented encouraging results from a study that looked at the acceptability of a long-acting cabotegravir/rilpivirine injection among people living with HIV.
A total of 611 people were randomly assigned to continue daily oral HIV medications or switch to once-monthly injections. The researchers were interested in the experiences of people who switched to the injections, and assessed things like injection pain, overall acceptability of the treatment and if they would recommend the injections to other people living with HIV.
Overall, participants gave high acceptability ratings to the long-acting injections. Over the course of the study, people who received the monthly injections had a 13.7-point improvement in acceptability scores (from baseline to week 48).
There were very few discontinuations throughout the course of the study, and only four people (out of 303) had injection site reactions that led to withdrawal.
Most participants (90%) reported that injection site reactions (e.g., swelling) were either “totally acceptable” or “very acceptable.” 86% of participants said that pain from injections were either “totally acceptable” or “very acceptable.”
Compared to people in the study who took daily oral medications, people who received the once-monthly injections scored more positively things like willingness to continue with the treatment, flexibility of treatment, convenience and willingness to recommend treatment.
“This indicates that the long-acting treatment meets participants’ expectations and supports the therapeutic potential of monthly dosing,” said Murray.
In April 2019, ViiV Healthcare applied for marketing approval to the U.S. Food and Drug Administration (FDA), and the FDA has set a target approval date of December 29, 2019. If approved, this treatment regimen would be the first-ever long-acting HIV treatment for people living with HIV.
Publication of the largest-ever study of the roles of genes in homosexual behavior is fanning the debate over whether being gay is due to genes or environment.
“There is no ‘gay gene’ that determines whether someone has same-sex partners,” says Andrea Ganna, a geneticist at the Broad Institute of MIT and Harvard and the University of Helsinki.
Family studies have suggested that genetics account for about 32 percent of heritability of homosexual behavior. But each SNP, or single nucleotide polymorphism, has a very small effect on whether someone has ever had a same-sex sexual partner, the new research found.
Taking into account all the SNPs measured in the study, including those that weren’t statistically significantly associated with same-sex behavior, explained only 8 to 25 percent of heritability of same-sex behavior. When considering just those five statistically significant SNPs, that number drops to much less than 1 percent.
But those variants could point to biological processes that are involved in choosing sex partners, the researchers say. For instance, one variant identified in the study has been linked to male-pattern baldness, and another to the ability to smell certain chemicals, which may affect sexual attraction.
“The study is a big step forward because of its huge size,” says J. Michael Bailey, a psychologist at Northwestern University in Evanston, Ill., who has worked on sexual orientation genetics but was not involved in the work. It included more than 470,000 people, dwarfing previous research.
“This is the first study that we can be pretty sure that they’ve identified genetic variants associated with an aspect of same-sex behavior,” Bailey says. “I’ve been a coauthor on some previous molecular genetic studies that were much more tenuous. I believe these results will replicate.”
But Bailey disagrees with some of the study’s conclusions. For instance, Ganna says that people who have exclusively same-sex or exclusively opposite-sex partners are genetically distinct from people who have partners of both sexes. That means that sexuality may not be a continuum from completely heterosexual to homosexual after all. So the Kinsey scale, which scores people’s sexual behavior along a spectrum with bisexuality in the middle, may need to be rethought, the researchers say.
But the Kinsey scale accurately predicts men’s arousal when shown erotic pictures of either men or women, Bailey says. That makes it a far better tool than the genetic score for predicting sexual preference, he says.
Qazi Rahman, a psychologist and sexual orientation researcher at King’s College London, has bigger quibbles with the study. “I should be really excited about this,” he says. But “despite being an ardent believer in the biological basis of sexuality, I’ve found this study problematic, and I’m not at all sure what was found and whether that holds up.”
Rahman points to what he sees as inconsistencies in the data and possible bias in the people who volunteered to participate in the study. The study drew volunteers from two big genetic databases, the UK Biobank and the consumer DNA testing company 23andMe, and from three smaller studies. Participants answered questionnaires about how many sexual partners of each sex they had ever had. 23andMe customers also responded to questions about attraction, sexual identity and fantasies.
But only 5.5 percent of UK Biobank participants and about 1.5 percent of 23andMe’s customers joined the study. Such low participation rates could skew the results, or point to genetic variants that make people more likely to sign up for a study. “What you’re getting is genetic influences on self-selection into a study, not genetic influences on same-sex behavior,” Rahman says.
It’s legitimate to question where study participants come from, but there’s no way to know whether that bias is affecting the results, says coauthor Benjamin Neale, a geneticist at Massachusetts General Hospital in Boston and the Broad Institute.
The study wasn’t designed to address sexual orientation or identity, but the same variants associated with same-sex behavior were also associated in 23andMe participants with attraction, sexual identity and fantasies. The small contribution of genetics to sexual behavior is in line with genetic contributions to other behaviors, such as level of education attainment. “There’s a lot of room for nongenetic effects,” Bailey says.
The authors don’t disagree. The study underscores that elements of both biology and one’s environment may play roles in shaping sexual behavior, Neale says. Environmental influences may include an array of developmental, social and cultural factors that all could affect behavior, he says.
That’s true, says coauthor J. Fah Sathirapongsasuti, a computational biologist at 23andMe in Mountain View, Calif. But, he says, “just because something is not completely genetic or something has an environmental, or what we call nongenetic, component doesn’t mean it’s a choice.”
There’s a new antiretroviral, from a new class of medication, currently being tested for both PrEP and HIV treatment. Named islatravir (formerly MK-8591), this Merck drug is showing promise as part of a novel drug delivery system and because of its long half-life, great potency and high barrier for resistance.
“It is clear that PrEP and HIV medication alternatives are evolving,” said Christopher Hall, MD, MS, AAHIVS, vice president of medical affairs at San Francisco AIDS Foundation. “More options are needed especially for PrEP, because a single agent will never meet the needs of all people. Personal choice certainly will take on greater significance as alternatives evolve.”
Islatravir in a PrEP implant
Based on a design similar to that used for the Nexplanon/Implanon birth control implant, the islatravir implant is a removable implant designed to be inserted under the skin in the upper arm for a year. In the study presented by Matthews, researchers tested the drug concentration levels delivered by the islatravir implant over 12 weeks in 16 individuals.
The implant device, with size shown relative to a penny. The implant is 4 cm in length x 2 mm. Photo courtesy of Merck.
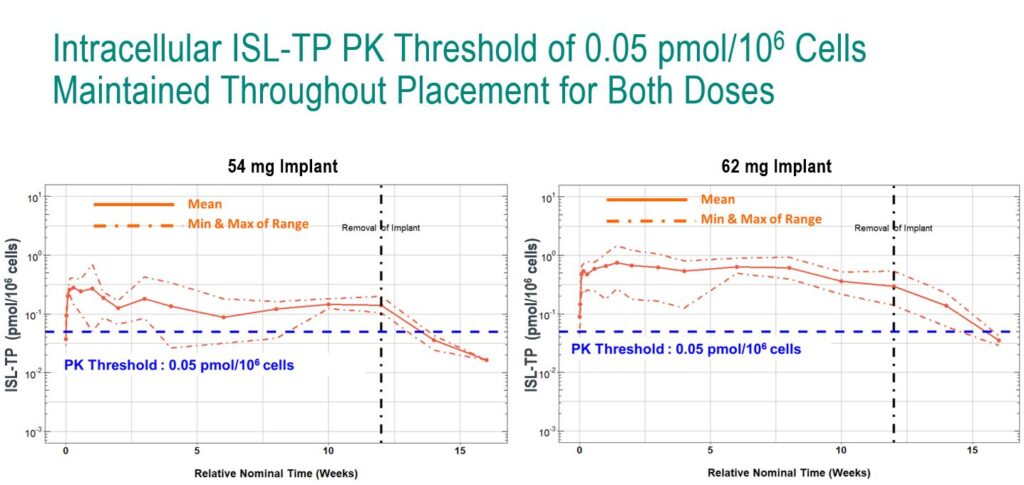
In a double-blind, placebo-controlled study, the researchers tested two doses of the islatravir implant: 54 mg and 62 mg. Throughout the study, the researchers collected drug concentration levels in plasma and PBMCs, and were primarily interested in how much time the drug concentration levels fell below a threshold of 0.5 pmol/106 (a threshold which is believed to provide an adequate level of drug for HIV prevention based on animal studies).
At both doses, drug concentrations remained above the 0.5 pmol/106 threshold for the 12 weeks of the study, although the lower limit of the estimated range for the 54 mg dose dipped below the threshold for a brief period. The 62 mg implant delivered drug concentration levels well above the threshold for the duration of the study.
In a later analysis, the researchers projected that the 62 mg implant would lead to concentrations above the threshold for at least 12 months, falling below the threshold at around 16 months.
Slide: Randolph Matthews, MD, PhD
“This supports the potential of the islatravir implant as a once-yearly PrEP option,” said Matthews.
Future research, he said, will continue to test other prototype implants and additional doses.
“Just as in birth control, implanted, long-acting pharmaceuticals are likely to earn a place in the biomedical HIV prevention armamentarium,” said Hall. “While more study is needed, clearly the future of PrEP is one of greater alternatives, with agents that bring fewer side effects, are less susceptible to resistance, are easier to administer, and improve the experience of people who take them. The future promises a broader array of options than we have seen since the advent of FDA-approved Truvada for PrEP in 2012, and it is bright.”
Islatravir for dual-therapy HIV treatment
There are a few unique characteristics of islatravir that may make it suitable as part of a two-drug regimen, said Molina. In preclinical studies, islatravir showed more than 10-fold greater potency compared to other approved antiretrovirals. The drug is also known to act against a number of resistant HIV variants, has a long half-life and has a high barrier to resistance.
“This [two-drug regimen] may maintain efficacy comparable to a three-drug regimen,” said Molina.
To test this, a double-blind study involving 120 treatment naïve adults living with HIV randomized participants to receive islatravir 0.25 mg, 0.75 mg, 2.25 mg or doravirine plus 3TC (lamivudine)/TDF (tenofovir disoproxil fumarate). At 24 weeks, or once viral loads were suppressed to <50 copies/mL on the triple-therapy, 3TC was removed.
There were very high response rates to the dual therapy at every dose level of islatravir.
After 24 weeks on the dual therapy, close to 90% of people receiving either islatravir 0.25, 0.75 and 2.25 mg with doravirine had viral loads <50 copies/mL. (96% of people receiving the control treatment of doravirine, 3TC and TDF had viral loads suppressed to this level.)
There were very few adverse events during the study, with two out of 90 participants receiving islatravir discontinuing the study because of adverse events.
“These results are quite promising, and demonstrate that the dual combination of islatravir and doravirine has the potential to be a potent, two-drug regimen and supports its further exploration in Phase 3 trials,” said Molina.
More research on islatravir’s safety and efficacy is needed before the drug may be granted FDA approval and brought to market. Based on the results of these studies, Merck plans to continue Phase 3 research on islatravir for HIV treatment as part of a once-daily, oral two-drug regimen. Using islatravir for PrEP, Merck is pursuing a Phase 2 study, set to begin enrolling in September 2019, that will evaluate the safety and tolerability of once-monthly oral islatravir.
An FDA advisory panel on Wednesday voted in favor of Gilead Sciences Inc’s combination drug to reduce the risk of sexually acquired HIV infection in men and transgender women who have sex with men.
The treatment, Descovy, is a combination of emtricitabine and tenofovir alafenamide, and is already approved to treat chronic HIV.
When asked to assess the efficacy of Descovy for pre-exposure prophylaxis (PrEP) of HIV in men and transgender women who have sex with men, a patient population that forms the largest component of the PrEP market, the panel voted 16-2 in favor.
The recommendation is a shot in the arm for Gilead as its third best-selling HIV drug, Truvada, faces exclusivity loss in the United States, beginning 2020.
Truvada is largely boosted by its PrEP use, SVB Leerink analyst Geoffrey Porges said in a note ahead of the committee’s discussion. “Truvada grew at 15% last year, entirely due to PrEP.”
Descovy’s entry into the still underpenetrated PrEP market is vital to Gilead’s attempts to retain its Truvada patient base after the drug goes off-patent, he said.
Truvada accounted for 20.5% of the drugmaker’s total HIV franchise sales in 2018.
The panel’s backing also comes as a possible launch of Descovy for PrEP faces opposition from patient advocacy groups.
They cite the scheduled U.S. launch next September of a generic version of the only currently approved prevention pill, Truvada, that could lower costs.
The panel, however, said there was not enough data to support the expansion of Descovy’s label for use as a preventive HIV drug for cisgender women. The panel voted 10-8 against its approval in this patient population.
Cisgender women form less than 7% of PrEP use and the prospect of Descovy’s label not including the population is not likely to impact the drug’s sales, Jefferies analyst Michael Yee said in a note ahead of the panel’s decision.
The FDA is yet to make a final decision on Descovy’s approval for PrEP. While the agency is not bound to follow the advice of its advisory panels, it usually does so.
In 1985, I was working in an STD clinic in Nashville, Tennessee, and was one of two HIV counselors doing pre-test and post-test counseling for people most likely getting the very first HIV test of their lives. There were NO anti-HIV medications available at that time, and the only ounce of hope you could impart to these newly infected people was that there appeared to be more HIV-positive (POZ) people not yet ill than there were POZ persons who were having symptoms. In 1985, untreated POZ people most likely had VERY high HIV viral loads (high amounts of active HIV virus in the body), were therefore very infectious and highly likely to pass HIV on to other sex or needle sharing partners.
In 2019, by contrast, we have a total of 51 medications at our disposal to fight HIV (33 individual anti-HIV meds and 18 combination anti-HIV meds). We are also finding that the majority of HIV patients consistently taking these anti-HIV meds have achieved undetectable levels of HIV in their bodies (defined as less than 200 copies/ml or a less than 200 HIV viral load). We know that current treatments are prolonging life for HIV POZ people. And in a true game-changer for the future of the epidemic , multiple studies have shown that HIV-positive people who are undetectable DO NOT transmit the virus to others!
A person is most infectious with the HIV virus during the first 3 months after they have been infected – if they are not taking meds. These newly HIV POZ persons often have a viral load between half a million to over TEN million in their blood, semen or vaginal fluids. The clinical implications of having a viral load of millions compared to having a viral load of under 200 are huge! That is why aggressive programs today seek to test people as early in HIV infection as possible, connect them to medical care and start them on anti-HIV meds as quickly as possible.
Across three different studies, including thousands of couples and many thousand acts of sex without a condom or pre-exposure prophylaxis (PrEP), no HIV transmissions to an HIV-negative partner were observed when the HIV-positive person was virally suppressed. This means that people who take anti-HIV meds daily, as prescribed, and who achieve and maintain an undetectable viral load have effectively NO risk of sexually transmitting the virus to an HIV-negative partner.” (U.S. Centers for Disease Control & Prevention (CDC),September, 2017)
Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases (NIAID), in an address he gave at a 2018 International AIDS Conference in Amsterdam, concluded “that the body of scientific evidence to date has established that there is effectively no risk of sexual transmission of HIV when the partner living with HIV has a durably undetectable viral load, validating the U=U [Undetectable = Untransmittable] message of HIV treatment as prevention.”
Results from the from recent PARTNER2 study, which only recruited gay couples, were presented in 2018. In total they documented 75,000 barrier-free instances of anal sexual intercourse between serodiscordant gay couples (one positive and one negative partner). The PARTNER study recruited HIV serodiscordant couples at 75 clinical sites in 14 European countries. They tested the HIV-negative partners every six to twelve months for HIV, and tested viral load in the HIV-positive partners. Both partners also completed behavioral study surveys. In cases of HIV infection in the negative partners, their HIV was analyzed to see if it came from their regular partner or if they had been with someone else.
The study found no transmissions between gay couples where the HIV-positive partner had a viral load under 200 copies/ml – even though there were nearly 75,000 acts of condomless sex between them. The results suggest, “A precise rate of within-couple transmission of ZERO” for gay men (a previous study had shown zero transmission in heterosexual couples). Dr. Alison Rodger (lead author of PARTNER2 study at the International AIDS Conference presentation- July, 2018) put it best when she said ”I just want to pay tribute to the U=U campaign. It has been astonishing. I think the time for excuses are over. I think it is very, very clear that the risk (of transmission) is zero. I very much think we have to promote this… if you are on suppressive on anti-HIV meds you are sexually non-infectious and the time for excuses is over.”
The latest HIV San Francisco epidemiology report shows that the number of new HIV diagnoses continues to decline, falling to 221 cases in 2017 — the lowest number since the start of the epidemic. This represents a five percent decline from 2016, following two years of steeper drops of around 15 percent. Much of this is attributed to more and more HIV POZ persons being on anti-HIV meds and being unable to transmit HIV. The increasing use PrEP, or pre-exposure prophylaxis, in which an HIV-negative person takes a daily anti-HIV med to block infection, is another reason.
In 2018, the statistics show that 92 percent of all HIV POZ Marin County residents (who are on HIV meds) have achieved undetectable viral loads. All of this important news isn’t just good for HIV prevention, but also for HIV POZ individuals. Every HIIV POZ person I know wants to avoid passing the virus on to others. It is important news for those who have not tested for HIV yet, or who have not started treatment yet, that becoming U=U can lift a huge burden of worry off of their shoulders. And finally, having HIV-NEGATIVE people know about U=U helps them to realize that they do not have to stigmatize and avoid HIV-POZ people!
I encourage you – please do everything you can to pass on this information regarding the U=U campaign, as it will help (a) encourage people to know their HIV status; encourage HIV POZ people to be taking meds and be adherent with their med schedules, reduce the stigma and fear directed toward HIV POZ persons; and help sero-discordant couples better navigate their relationships without fear.
Dave Brown formerly worked with the Centers for Disease Control, US Public Health Service
The global fight against AIDS is stalling due to lower investment, marginalized communities missing vital health services, and new HIV infections rising in some parts, the United Nations warned on Tuesday.
More than half of all new HIV infections in 2018 were among sex workers, drug users, men who have sex with men, transgender people, prisoners and the sexual partners of these groups, according to a report by UNAIDS. Many of those populations did not get access to infection prevention services, it said.
Progress in some countries has been “impressive,” the U.N. body’s report said, but others are seeing rising numbers of HIV infections and AIDS-related deaths.
It noted “worrying increases” in new infections in eastern Europe and central Asia, where HIV cases rose by 29 percent, as well as in the Middle East, North Africa and Latin America.
“Ending AIDS is possible if we focus on people not diseases,” said UNAIDS Executive Director Gunilla Carlsson.
She said now was the time to “create road maps for the people and locations being left behind (and) take a human rights-based approach to reaching people most affected by HIV.”
This would need greater political leadership, she said, starting with adequate and well-targeted investment.
Global funding for the AIDS fight dropped off significantly in 2018 – by nearly $1 billion – as international donors gave less and domestic investments did not grow fast enough to plug the gap. Around $19 billion was available for the AIDS response in 2018, UNAIDS said – falling $7.2 billion short of the total $26.2 billion it says is needed by 2020.
Globally in 2018, some 770,000 people died of AIDS and almost 38 million people were living with the human immunodeficiency virus (HIV) that causes it.
HIV cannot be cured but the infection can be kept in check by AIDS drugs known as antiretrovial treatment.
Around 23.3 million of the 37.9 million people with HIV worldwide currently get the AIDS drugs they need.
Around 1.7 million people were newly infected, the UNAIDS report said, a 16% decline since 2010, driven mostly by steady progress in parts of eastern and southern Africa.
South Africa, for example, has cut new HIV infections by more than 40% and AIDS-related deaths by around 40% since 2010.
But the report warned there is still a long way to go in many parts of eastern and southern Africa – the regions most affected by HIV.
As pre-exposure prophylaxis (PrEP) gains acceptance, medical experts and policymakers are finding new ways to make this effective HIV prevention tool accessible to more people who could benefit.
Last month the California Senate passed a bill that will allow pharmacists to provide PrEP and post-exposure prophylaxis (PEP) without a prescription. And in June, the U.S. Preventive Services Task Force (USPSTF) recommended that health care providers offer PrEP to people at risk of acquiring HIV, paving the way for broader insurance coverage.
PrEP at the Pharmacy
SB 159, co-authored by Senator Scott Wiener (D-San Francisco) and Assemblymember Todd Gloria (D-San Diego), authorizes pharmacists to offer a month’s worth of PrEP or a course of PEP without prescription from a physician. It also prohibits insurance companies from requiring prior authorization for PrEP coverage.
On May 21, the Senate approved the bill by a wide 34-to-1 margin, sending it on to the Assembly.
“By allowing pharmacists to furnish these revolutionary medications, we will help reduce HIV infection rates and create a stronger path toward ending new HIV infections entirely,” Wiener said. “We have the tools to end new HIV infections, and we can get there in our lifetime.”
San Francisco AIDS Foundation (SFAF) co-sponsored the bill and was involved in the process of moving it forward, said Courtney Mulhern-Pearson, senior director of policy and strategy.
“The goal of the bill is to make PrEP accessible at a point when people are willing and able to start,” she said. “We’re looking at PrEP uptake and realizing we need to do more to increase access across the state. This is an innovative way to increase access to and awareness of PrEP and to make sure it’s available to all who need it.”
The bill’s current language allows pharmacists to provide a 30-day supply of Truvada (tenofovir disoproxil fumarate/emtricitabine) PrEP to individuals who have had a negative HIV test within the previous seven days. The client would then be referred to a medical provider for the recommended monitoring, including screening for sexually transmitted infections (STIs) and kidney function tests. Pharmacists would also be able to offer a month-long course of PEP, which can prevent HIV infection if started within 72 hours after exposure to HIV.
Some have raised concerns about providing PrEP without testing kidney function in advance, because the tenofovir in Truvada could potentially cause kidney impairment in susceptible individuals. But studies have shown that kidney problems are uncommon among people using Truvada for HIV prevention.
“One month is not going to be a problem,” according to Robert Grant, MD, of the University of California at San Francisco, who led a major study showing that PrEP is highly effective for gay and bisexual men. “We’re not seeing kidney problems very much at all in people seeking PrEP. These typically occur four to five months after starting and they’re rare.”
“We’re only providing PrEP to a small proportion of people who could benefit, and making it more accessible and more convenient at pharmacies will be a step toward stopping HIV transmission,” Grant added.
The Centers for Disease Control and Prevention estimated that less than 10% of the more than 1.1 million people at high risk for acquiring HIV were using PrEP as of 2015. The numbers were even lower for African Americans (1%) and Latinx people (3%), who have high rates of new HIV infections. In California, the state Office of AIDS estimates that as many as 240,000 Californians could be eligible for PrEP, but only around 9,000 people were using it as of late 2016.
“The low rates of PrEP and PEP use across California signal the need to offer these effective prevention tools in additional ways,” said SFAF CEO Joe Hollendoner. “This bill removes unnecessary barriers and streamlines access to PrEP and PEP, so anyone who needs preventative measures can get them.”
USPSTF Recommendation
The new USPSTF recommendation for PrEP carries an “A” grade, meaning it is well-supported by scientific evidence. The Affordable Care Act requires insurers to cover preventive recommended services with an “A” or “B” rating.
“The new recommendation for PrEP is enormously important news for the struggle against HIV,” said Grant. “This grade A recommendation reflects the available evidence, which strongly supports the use of PrEP as a safe, effective method of HIV prevention.”
As described in a June 11 statement in the Journal of the American Medical Association, the recommendation says that clinicians should offer PrEP to sexually active men who have sex with men (MSM) and heterosexual women and men who have an HIV-positive sex partner, do not use condoms consistently, or have had an STI within the past six months. PrEP is also recommended for people who injection drugs who share needles or other injection equipment.
Although few transgender people have been included in trials, PrEP has been shown to reduce the risk of acquiring HIV through receptive or insertive anal or vaginal sex, so it can be considered for cisgender and transgender people alike, according to the authors.
The task force experts recommend once-daily Truvada—currently the only PrEP regimen approved by the Food and Drug Administration—for all at-risk groups. But it also says that tenofovir disiproxil fumarate alone, which is available as an inexpensive generic, is an option for heterosexual men and women and people who inject drugs, based on studies showing that it lowers HIV risk in these groups. No equivalent studies with MSM have been done.
The new recommendation has the potential to substantially expand access to PrEP. Many private insurers already cover Truvada for HIV prevention—which is priced at around $1,600 per month—but cost sharing is common. Gilead Sciences offers a co-pay card that people with private insurance can use to cover out-of-pocket costs, but some claim this benefit is inadequate. Many state Medicaid programs, including California’s, cover PrEP, but this represents a substantial public financial burden given competing funding needs.
Expanding PrEP use among people who need it most will also require raising awareness and combatting stigma.
“PrEP has been proven to be a highly effective intervention in preventing new cases of HIV, and receiving an A grade is an important step towards increased access,” Hollendoner said. “We know, however, that access alone does not result in utilization, so we call on healthcare providers to educate their patients who are at risk for HIV acquisition—especially those who are people of color—about PrEP and how it can protect their sexual health.”