While the One Male Condom is not markedly different from the hundreds of other condoms on the market, it is the first that will be allowed to use the “safe and effective use” label for reducing sexually transmitted infections during anal sex. It is also approved for use as a contraceptive and as a means to reduce STIs during vaginal intercourse.
“This landmark shift demonstrates that when researchers, advocates, and companies come together, we can create a lasting impact in public health efforts,” Davin Wedel, president and founder of Boston-based Global Protection Corp, maker of the One Male Condom, said in a statement. “There have been over 300 condoms approved for use with vaginal sex data, and never before has a condom been approved based on anal sex data.”
Courtney Lias, director of the FDA’s Office of GastroRenal, ObGyn, General Hospital and Urology Devices, noted that the risk of STI transmission during anal intercourse is “significantly higher” than during vaginal intercourse.
“The FDA’s authorization of a condom that is specifically indicated, evaluated and labeled for anal intercourse may improve the likelihood of condom use during anal intercourse,” Lias said in a statement. “Furthermore, this authorization helps us accomplish our priority to advance health equity through the development of safe and effective products that meet the needs of diverse populations.”
Anal sex poses the highest risk for contracting HIV, with the risk of HIV transmission from receptive anal sex about 18 times higher than receptive vaginal sex. Gay and bisexual men accounted for 69 percent of the 36,801 new HIV/AIDS diagnoses in the U.S. in 2019, according to the Centers for Disease Control and Prevention. Queer men of color were overrepresented within this group, with Black men representing 37 percent, Latino men representing 32 percent and white men representing 25 percent of these new diagnoses, according to the CDC.
One Male Condoms are available in standard, thin and fitted versions, and the fitted version is available in 54 different sizes.
A clinical trial of 252 men who have sex with men and 252 men who have sex with women found the One Male Condom has a failure rate of 0.68 percent for anal sex and 1.89 percent for vaginal sex, according to the FDA, which defined condom failure as condom slippage or breakage.
Dr. Will DeWitt, clinical director of anal health at the Callen-Lorde Community Health Center in New York City, said the newly approved condoms could be a helpful tool for HIV/AIDS prevention.
“The hope would be that people would be more willing to use condoms for anal sex and to have that direct encouragement would increase the rates of people using them,” DeWitt said. “Condoms still remain an important tool for people who don’t want to or can’t use PrEP.”
PrEP, or pre-exposure prophylaxis, is typically taken in the form of a daily pill to prevent HIV/AIDS in people who are not diagnosed with the virus. Last year, the FDA also approved an injectable PrEP shot that can be given every two months.
DeWitt did, however, add that he is worried the One Male Condom name and marketing could alienate those who engage in anal sex but do not identify as male.
“Anal sex really does belong to everyone,” DeWitt said. “Even if it’s the perspective of who has to wear the condom, it’s not just male bodies and male identified folks who need to use it.”
While health experts have long encouraged the use of condoms for STI prevention through anal sex, DeWitt said FDA’s official approval is long overdue.
“Here we are in 2022, and we are only now getting condoms approved for anal sex,” DeWitt said, noting that it’s been more than three decades since the start of the HIV crisis. “It’s a little frustrating that it’s taken this long to have this kind of official endorsement.
A trans teen died by suicide while waiting to access mental health care and a first appointment at a gender identity clinic, with a coroner warning that future deaths are possible unless action is taken.
Daniel France, a 17-year-old teenager from Cambridgeshire, killed himself during the first coronavirus lockdown in April 2020 while taking medication to treat depression.
He was trans, and had been referred to an NHS gender clinic – but, like thousands of others, faced several years of waiting before he would be called for his first appointment.
France, described as “extremely kind” and someone who had “many friends” by a local LGBT+ group, also had a history of suicide attempts, said coroner Philip Barlow.
In a report to “prevent future deaths” following an inquest into France’s suicide, Barlow told local agencies to address the delays in accessing mental health services for young adults, and noted concerns around the waiting times for NHS gender clinics.
“Danny was a vulnerable teenager,” Barlow wrote in his coroners report, adding that two separate safeguarding referrals to Cambridgeshire County Council about France had been “incorrectly” closed.
According to the report, France sought counselling from the NHS’ Improving Access to Psychological Therapies (IAPT) programme, but was deemed too high risk. When he was assessed by Cambridge’s First Response Service, which supports people experiencing a mental health crisis, it was decided he did not ‘require urgent intervention’. He had been referred to adult mental health services, having previously been under a young person’s service, but was still awaiting assessment.
The coroner noted that France “was repeatedly assessed as not meeting the criteria for urgent intervention” and that the “waiting list for psychological therapy was likely to be over a year from point of first presentation”.
The inquest also heard “evidence about the considerable delay in obtaining appointments for the Gender Identity Clinic, and about the shortage of availability for psychological therapies such as CBT”.
Barlow warned: “In my opinion there is a risk that future deaths could occur unless action is taken.”
A copy of Barlow’s coroners report has been sent to NHS England and the secretary of state for health, Sajid Javid “for information purposes only”. The local council and NHS trust have been given 56 days to respond to Barlow’s concerns on mental health care provision
The Kite Trust, a local charity that runs support groups for young LGBT+ people that France attended, warned about the “hostile society” that trans people, and especially young trans people, currently face in the UK.
“What Danny faced, and what trans people of all ages continue to face, is a society that is hostile to our very existence,” said Pip Gardner, chief executive of The Kite Trust, in an emailed statement. “Using the wrong name or pronouns for a trans person, is not just a spelling mistake – it causes emotional harm and breaks down trust.”
They continued: “The responsibility must be on those with statutory duties and in positions to safeguard young people’s welfare, especially crisis services, to take immediate action to ensure that other trans young people like Danny can access the care they are entitled to, without having to endure such harms.”
Suicide is preventable. Readers who are affected by the issues raised in this story are encouraged to contact Samaritans on 116 123 (www.samaritans.org), or Mind on 0300 123 3393 (www.mind.org.uk). Readers in the US are encouraged to contact theNational Suicide Prevention Line on 1-800-273-8255.
A study has found that COVID-19 vaccine rates in the United States are higher among gay and lesbian adults than in heterosexual adults.
The Centre for Disease Control and Prevention (CDC) found that lesbians and gay men aged 18 and older reported higher levels of vaccine coverage (85.4 per cent) than their straight counterpoints (76.3 per cent).
It was found that bisexual (76.3 per cent) and transgender adults (75.7 per cent) had similar COVID-19 vaccine rates to heterosexual people.
The study authors explained that the data could help to “increase vaccination coverage”.
The authors said: “Understanding COVID-19 vaccination coverage and confidence among LGBT+ populations, and identifying the conditions under which disparities exist, can help tailor local efforts to increase vaccination coverage.
“Adding sexual orientation and gender identity to national data collection systems would be a major step toward monitoring disparities and developing a better-informed public health strategy to achieve health equity for the LGBT+ population.”
According to CDC researchers, people within the LGBT+ community “have higher prevalences of health conditions associated with severe COVID-19 illness compared with non-LGBT populations”, for example obesity, smoking, and asthma.
A previous study explained: “Because of their sexual orientation, sexual minority persons experience stigmatisation and discrimination that can increase vulnerabilities to illness…
“Persons who are members of both sexual minority and racial/ethnic minority groups might therefore experience a convergence of distinct social, economic, and environmental disadvantages that increase chronic disease disparities and the risk for adverse COVID-19–related outcomes.”
Sia Sehgal, a student at a private international school outside Mumbai, raised 200,000 rupees (£1,933) for the Maharashtra District AIDS Control Society (MDACS) to buy COVID-19 vaccines.
MDACS administered 120 first doses to trans people during a free vaccination drive in July last year.
Varshabhai Dhokalia, a trans woman, told the Hindustan Times after receiving the free vaccine: “We are always being mocked. While I was standing in the queue for the shot, people were staring and laughing at me. Someone even passed a comment that the vaccination was only for males and females.
“This discourages us from going to these centres for vaccination.”
Sehgal raised the money for the 120 first COVID-19 vaccine doses in two weeks, and planned to raise more funds so that the people who had their first vaccine could have their second.
More than 1 in 4 LGBTQ youth have experienced homelessness or housing instability at some point in their lives, a new report from The Trevor Project shows, including nearly half of Native/Indigenous LGBTQ youth and nearly 40 percent of transgender and nonbinary youth.
Thirty-five percent of LGBTQ youth who are homeless and 28 percent who have experienced housing instability also reported a suicide attempt in the last year, compared to 10 percent of LGBTQ youth who are not housing insecure. Homeless LGBTQ youth are also two to four times more likely to report depression, anxiety, self-harm, suicidal thoughts and suicide attempts.
These findings, said Jonah DeChants, one of the authors of the study and a research scientist for The Trevor Project — an LGBTQ youth crisis intervention and suicide prevention organization — “paint a pretty serious picture about the need to provide better mental health services for folks who are experiencing housing instability.”
It came as no surprise to the researchers that LGBTQ youth of color and trans and nonbinary youth are disproportionately affected by homelessness and mental health issues.
“When you start adding homophobia, plus racism or transphobia, plus anti-Indigenous racism,” DeChants said, “then we again start to see that young people who are experiencing multiple forms of marginalization and oppression — those are the folks who tend to be pushed out of housing supports and experiencing homelessness.”
Experts say the pandemic has also exacerbated housing and mental health concerns. Last year more than 80 percent of LGBTQ youth reported that the pandemic has worsened their housing situations, according to The Trevor Project’s 2021 National Survey on LGBTQ Youth Mental Health.
“Nothing repairs the damage that is typically done by being rejected by your family, your community, the culture at large,” Bill Torres, director of drop-in support services at the Ali Forney Center in New York, one of the largest LGBTQ youth homeless shelters in the U.S., said. “In regards to the impact of how Covid is affecting everyone, it just increased those issues tenfold.”
Kate Barnhart, the executive director of New Alternatives, a drop-in crisis center for homeless LGBTQ youth and people living with HIV in New York, said the hopelessness of the pandemic is driving some suicides among clients.
“We’re seeing people who’ve gotten disconnected from their medical and their mental health services,” Barnhart said. “Telehealth is fine if you’re middle class, but if you don’t have a device, or you don’t have Wi-Fi or you’re in an eight-man room at the shelter, and you don’t have the privacy to talk to your psychiatrist … that doesn’t work that well.”
Researchers note that the passage of LGBTQ nondiscrimination protections and LGBTQ competent housing programs can help close the gaps in care.
Elisa Crespo, the executive director of the New Pride Agenda, an LGBTQ advocacy group, advised that increased access to employment and permanent housing can also help LGBTQ young adults who are experiencing homelessness.
“That means putting funding behind the implementation and education process of the policies that may already exist — so that not only young people understand their rights and protections, but housing providers understand as well,” Crespo said.
If you or someone you know is in crisis, call the National Suicide Prevention Lifeline at 800-273-8255, text HOME to 741741 or visit SpeakingOfSuicide.com/resources for additional resources.
The UK has seen a sharp rise in an “extremely drug-resistant” strain of the STI shigella among gay and bisexual men, according to a government report.
Although not well-known, a shigella infection, from a bacterium that causes dysentery, can be very serious.
Shigella is transmitted through the accidental ingestion of faecal matter containing the bacteria, such as by licking skin, condoms, toys or fingers that have been contaminated during rimming, fisting, or giving oral sex after anal sex. Even a tiny amount can cause infection.
The infection affects the gut, and can cause severe and long-lasting diarrhoea, stomach cramps and a fever. Because of its symptoms, it is sometimes mistaken for food poisoning.
The symptoms of shigella usually subside within a week, but in some cases hospitalisation is required to administer intravenous antibiotics. Rarely, shigella can spread to the blood and become life-threatening.
On Thursday (27 January), the UK Health Security Agency (UKHSA) reported that cases have been on the rise among gay and bisexual men,
In the last four months, the agency has recorded 47 cases of the STI, while in the 17-month period between April 2020 and August 2021, there were just 16 cases.
The UKHSA said that “recent cases show resistance to antibiotics is increasing”.
Dr Gauri Godbole, a consultant medical microbiologist at UKHSA, said in a statement: “Practising good hygiene after sex is really important to keep you and your partners safe. Avoid oral sex immediately after anal sex, change condoms between anal or oral sex and wash your hands with soap after sexual contact.”
She said it was vital that men who have sex with men speak to a GP or sexual health clinic if they experience symptoms so they can be tested for shigella, which is usually done via a stool sample.
“Men with shigella may have been exposed to other STIs including HIV, so a sexual health screen at a clinic or ordering tests online is recommended,” Godbole continued.
“If you have been diagnosed with shigella, give yourself time to recover. Keep hydrated and get lots of rest.
“Don’t have sex until seven days after your last symptom and avoid spas, swimming, jacuzzis, hot tubs and sharing towels as well as preparing food for other people until a week after symptoms stop.”
As of early this week, the U.S. Food and Drug Administration had yet to respond to a Nov. 29 joint letter by 52 members of the U.S. House and U.S. Senate calling on the FDA to end its policy of restricting the donation of human tissues such as corneas, heart valves, skin, and other tissue by men who have sex with men, or MSM.
The letter is addressed to Acting FDA Commissioner Janet Woodcock and Department of Health and Human Services Secretary Xavier Becerra. The FDA is an agency within the HHS.
The letter says the FDA’s restrictions on MSM tissue donation date back to a 1994 U.S. Public Health Service “guidance” related to the possible transmission of HIV, which stated that any man “who has had sex with another man in the preceding five years” should be disqualified from tissue donation.
“We also call your attention to the broad consensus within the medical community indicating that the current scientific evidence does not support these restrictions,” the letter states. “We have welcomed the FDA’s recent steps in the right direction to address its discriminatory MSM blood donation policies and urge you to take similar actions to revise the agency’s tissue donation criteria to align with current science so as not to unfairly stigmatize gay and bisexual men.”
The letter adds, “In fact, a recent study in the medical journal JAMA Ophthalmology estimated that between 1,558 and 3,217 corneal donations are turned away annually from otherwise eligible donors who are disqualified because of their sexual orientation, an unacceptable figure given widespread shortages of transplantable corneas.”
The letter continues, saying, “FDA policy should be derived from the best available science, not historic bias and prejudice. As with blood donation, we believe that any deferral policies should be based on individualized risk assessment rather than a categorical, time-based deferral that perpetuates stigma.”
U.S. Sen. Tammy Baldwin (D-Wisc.), the nation’s only out lesbian U.S. senator, and U.S. Rep. Joe Neguse (D-Colo.) are the two lead signers of the letter. All 52 signers of the letter are Democrats.
Among the others who signed their names to the FDA letter are four of the nine openly gay or lesbian members of the U.S. House. They include Reps. David Cicilline (D-R.I.), Richie Torres (D-N.Y.), Mondaire Jones (D-N.Y.), and Mark Takano (D-Calif.).
Also signing the letter are D.C. Congressional Del. Eleanor Holmes Norton (D-D.C.), and Rep. Jamie Raskin (D-Md.).
In response to a Dec. 21 email inquiry from the Washington Blade, FDA Press Officer Abigail Capobianco sent the Blade a one-sentence statement saying, “The FDA will respond to the letter directly.”
The statement didn’t say to whom the FDA would respond or when it would issue its response.
Using gender-neutral pronouns makes people more positive towards women and LGBT+ people and less biased towards men, scientists say.
Three experiments were carried out to determine the effects of using gender-neutral pronouns on people’s perception’s of women and LGBT+ people.
The results show that “individual use of gender-neutral pronouns reduces the mental salience of males.”
“This shift is associated with people expressing less bias in favour of traditional gender roles and categories, as manifested in more positive attitudes toward women and LGBT individuals in public affairs,” the research, published in the Proceedings of the National Academy of Sciences (PNAS), says.
Efrén Pérez, one of the authors of the study who is a political sciences professor at the University of California in Los Angeles, told The Guardian, “Let’s assume there are societies that generally agree on being more inclusive of women and LGBT individuals, and there are more than a few.”
“Our findings suggest that the words we choose to use can matter in getting us a little bit closer toward reaching that ideal.”
More than 3,000 people took part in the research, which involved being shown a cartoon of an androgynous figure walking a dog and then asked what was happening in the picture – with one group told to use only neutral pronouns, one female pronouns and one male.
Participants then completed tasks, including writing a story about a person running for political office and answering questions about their views on women and LGBT+ people.
According to the report, using gender-neutral pronouns at the beginning of the task made it more likely that the volunteers would use non-male names in their short story and would have pro-women, pro-LGBT+ views.
Sabine Sczesny, a professor of social psychology at the University of Bern who was not involved in the research, told The Guardian that the research was further evidence that gender-inclusive language could reduce gender-biases and “contribute to the promotion of gender and LGBT equality and tolerance.”
Laura Russell, director of research, policy and campaigns at Stonewall, said, “The language we use is important, especially when it comes to describing or referencing someone’s identity.
“This study adds to the evidence showing that when we use language that actively includes women and LGBT people, it makes a real difference in reducing gender stereotyping. Using gender-neutral language is a positive step towards creating a world where everyone is accepted without exception.”
We are lesbians and collaborators in the LGBTQ+ movement. We also have a third thing in common: We are both survivors of breast cancer. Each of our health journeys have led us to unite around a common goal to ensure that LGBTQ+ communities have what they need when facing a breast cancer diagnosis or getting treatment to prevent it.
In Dina’s case, she spent years undergoing countless procedures to mitigate her high breast cancer risks. She endured invasive surgeries that required grit, determination, resilience, and continual love and nurturing from her wife, Dom, their children, and their respective families. It went on for more than a decade.
Along the way, Dina also sought out support groups to help her cope with the emotions that arose around the bodily changes that resulted from her intense treatments. There, she faced a rude awakening. All of those groups were filled with straight women who did not react well when she spoke of her wife and her overall experience as a lesbian facing major breast health issues. In one online group, all but one of the women dropped off the call, after she shared insights from her LGBTQ+ perspective.
In another conversation, when Dina shared her sorrow over the loss she was feeling after a double mastectomy, the person she confided in quipped: “Well at least there’s still one set of boobs in your relationship,” referencing Dina’s wife, Dom, who has not faced any breast health problems herself. These incidents of insensitivity and misguided reactions left Dina feeling lonely, isolated, depressed, and unsupported.
Yet even as she rode the wave of these feelings, she felt a sense of resolve, knowing she had the skills, the contacts, and the wherewithal to make a change. As a registered nurse, author, DEI (diversity, equity, and inclusion) expert, and CEO of her own health care consulting firm, she set out to give LGBTQ+ people a new resource. She enlisted Cindi’s advice as a breast cancer survivor, LGBTQ+ public relations pro, and friend.
Cindi overcame the immense challenge of major breast cancer treatment in 2018 and 2019, penning this op-ed for The Advocate at the time about the disparities facing LGBTQ+ people with cancer. She shared important statistics in the piece from the National LGBT Cancer Network and looked to the future about how to use her experience as a catalyst for giving back. The piece also highlighted how lucky she was to have good insurance, health care providers who respected her identity, and an amazing support system (including, most importantly, her wife, Rainie) to move through the difficulties. Far too many LGBTQ+ people with cancer lack these privileges.
Today, we, Dina and Cindi, are both healthy and thriving. So, during Breast Cancer Awareness Month, we are thrilled to announce that we have formed a new nonprofit to fill the resource gap for those in our communities who are confronted with breast health challenges. It’s called the Inclusive Community for Breast Health or as we affectionately call it, “I See Breast Health,” a play on our acronym. ICBH will provide education and resources for LGBTQ+ individuals who are in treatment for, or seeking to prevent, breast cancer, and work to build cultural competence within the health care system through collaboration with academic and health organizations.
As Dina saw firsthand during her own nursing education, there is a dearth of information on LGBTQ+ populations for those being trained as nurses, doctors, and other health care roles. ICBH plans to formally partner with academic institutions and engage with current medical students and future health care providers so they have the tools they need to provide excellent breast-focused healthcare for LGBTQ+ people. Some of these collaborations have informally begun.
And although we are only just beginning our work, we’re excited to share a non-research based survey focused on identifying LGBTQ+ community support needs in the area of breast/chest health. The responses we receive will help us understand what people are facing so we can better focus our programming priorities to meet those needs. We’re also organizing our first online educational panel that will include a variety of LGBTQ+ individuals with varying experiences and perspectives on breast health. That event is planned for November and we will share specific details on our social media pages in the near future.
We are grateful to take these first steps in launching what we believe will be a vital source of information for LGBTQ+ individuals with breast health concerns. We aim to create a safe space for those in our communities who are in the midst of these circumstances and looking for help. We want to give them the freedom to be fully authentic as they seek guidance and community support. We’re excited to lay the groundwork and start executing our programming in earnest over the next year, and we look forward to reporting back to you about our progress during Breast Cancer Awareness Month in 2022.
Dina Proto, RN, is the Founder and CEO of Dina Proto International, a DE&I and LGBTQ+ Cultural Competency Consulting firm. In addition to her DE&I Healthcare Consulting firm, Dina is a Published Author, Speaker and Educator. In her book, Identity Impact: When Society’s Expectations Collide with the Authentic Self, Dina explores the clinical correlation between society’s projection of gender role and identity and healthcare disparities.
Cindi Creager is a media consultant with decades of communications experience in the news industry and LGBTQI non-profit world, including a successful tenure at ABC News, GLAAD, and her co-owned boutique public relations firm, CreagerCole Communications LLC.
A UK cervical screening pilot programme for trans men and non-binary people was so successful it could be used as a model for programmes around the world.
The pilot programme was launched in October 2019 in conjunction with the NHS as part of a study to address cervical cancer in trans and non-binary communities.
It offered weekly cervical screening clinics, only staffed by healthcare professionals with experience in treating trans and non-binary patients.
Of those who attended the clinic and gave feedback, 100 per cent were satisfied with the service, and a majority (60 per cent), said they would not have been screened if it were not for the clinic.
In the UK, screening is recommended every three years for all people with a cervix between the ages of 25 and 49, and every five years for those between age 49 and 64.
“Trans men and non-binary people are often reluctant to receive cervical screening, raising their risk of undetected human papillomavirus [HPV], which could lead to cervical cancer,” said Alison May Berner, a specialty trainee and clinical research fellow in medical oncology at Barts Cancer Institute in London, a specialist registrar with the Tavistock and Portman Gender Identity Clinic and the study’s lead author, per News Medical.
The results of the study were presented at the American Association for Cancer Research’s Conference on the Science of Cancer Health Disparities in Racial/Ethnic Minorities and the Medically Underserved this month, indicating that it could have international implications, and Berner said she wants further research to look at trans-specific cervical screenings in a GP setting.
She said: “People assume that this population’s health care-related needs are solely related to transition. That’s not true.
“Trans and non-binary people are at risk of HPV infection and cervical cancer if they continue to retain a cervix, and they stand to benefit from programs designed specifically for them.
“If you’re a trans or non-binary person living in a place where these specialist services do not exist, I would encourage you to work with a trusted health care professional to build relationships and ensure that you get the appropriate screenings, while continuing to have your identity respected.”
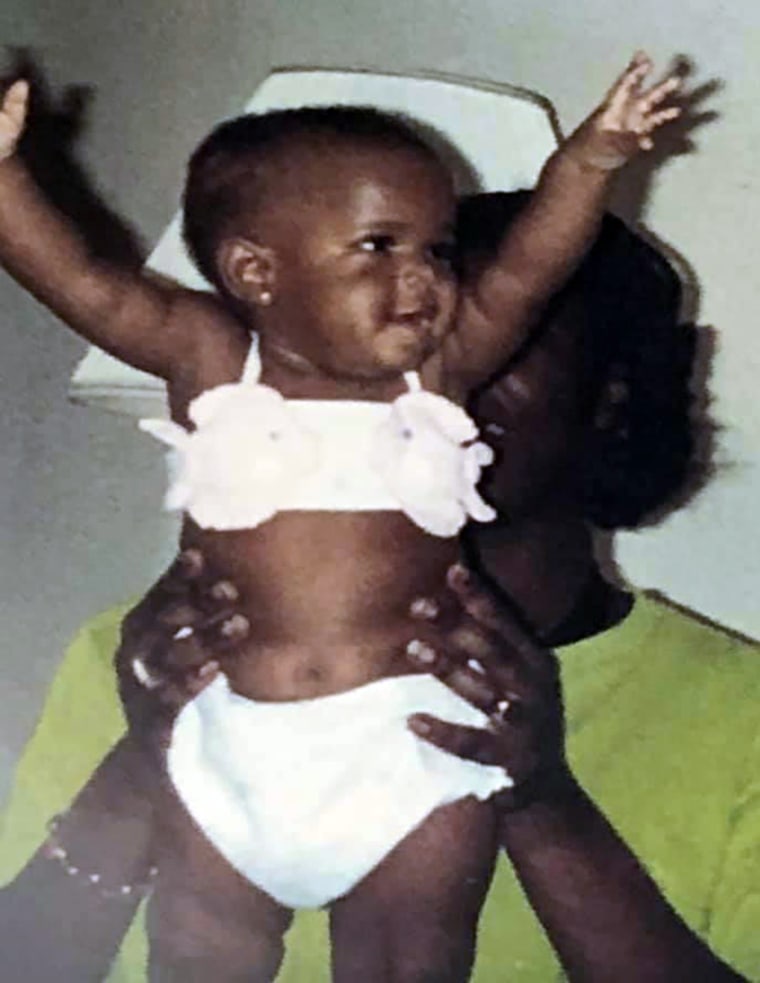
Bria Brown-King, 29, a Pennsylvania native, was raised as a girl. As Brown-King got older, however, they realized they were developing differently.
“I didn’t have the feminizing puberty that the other girls in my class had,” said Brown-King, who was born with an enlarged clitoris and started to develop masculine traits during puberty, including facial hair and larger muscles.
Brown-King, who has since come out as nonbinary and uses gender-neutral pronouns, was born with congenital adrenal hyperplasia, or CAH, a rare condition in which the body produces high levels of androgens — hormones that influence masculine characteristics. Those with CAH are considered intersex, an umbrella term used to describe individuals whose sex characteristics do not match strictly binary definitions of male or female. While rare, at least 1 in 2,000people are born with a genital difference caused by an intersex trait, according to Human Rights Watch, an international research and advocacy group.
Bria Brown-King.Courtesy Bria Brown-King
Though many children with CAH undergo “gender-normalizing surgery” to make the genitals look more typically female in infancy, Brown-King’s parents decided to wait until Brown-King was old enough to choose. But Brown-King said severe bullying over their appearance drove them to get the surgery at 13. Looking back, Brown-King, who now works for InterAct, an intersex advocacy group, said they would have made a different choice “had I known that it was OK to have the body that I had.”
These so-called gender-normalizing surgeries have been performed on intersex babies and toddlers since at least the 1950s — usually in secrecy, without ever telling the children when they get older. Until recently, doctors saw a genital difference as a “psychosocial emergency” and rushed to assign a gender and perform surgery, believing children would be psychologically harmed otherwise, according to Dr. Sue Stred, a retired pediatric endocrinologist who has worked with intersex youth for nearly three decades. Emergency surgery, however, is only necessary in rare cases — if a child can’t urinate properly, for example, according to medical experts who work with these children.
The exact number of hospitals that currently perform these surgeries is unknown, and only a handful specialize in such procedures. Adults who underwent these surgeries as children report mixed feelings, with many saying they have had no problems, while others say they are “just wrought with devastation” over complications, according to Kyle Knight, a senior researcher who interviewed dozens of intersex people for Human Rights Watch. Complications can include sexual dysfunction, loss of sensation, infertility and gender dysphoria, according to the report.
As more people tell their stories, an increasing number of organizations have condemned medically unnecessary surgeries on intersex youth, including the United Nations, the World Health Organization, Physicians for Human Rights, the American Academy of Family Physicians, Human Rights Watch and Amnesty International. Under mounting pressure, several hospitals have recently announced they would defer certain medically unnecessary genital surgeries until children are old enough to participate in the decision, including Lurie’s Children Hospital in Chicago, Boston Children’s Hospital and New York City Health & Hospitals, the largest public health care system in the United States.
“We empathize with intersex individuals who were harmed by the treatment that they received according to the historic standard of care and we apologize and are truly sorry,” Lurie Children’s Hospital announced in a statement last year. It was the first time a hospital had ever made such an apology.
‘The right answer right now isn’t clear’
There is fierce disagreement among doctors and advocates over whether surgical delays should extend to those with congenital adrenal hyperplasia. Unlike many other intersex youths whose genetics and reproductive organs make it difficult to assign a sex, those with CAH have distinctly male or female chromosomes and sex organs — and only those assigned female at birth undergo surgery because of genital and hormonal differences.
As such, some people who work with these children wonder if delaying surgery would do more harm than good. Even adults with CAH are divided over this. A recent study from Europe, which surveyed 459 intersex adults who underwent genital surgery as children, found that 66 percent of those with CAH thought infancy or childhood was an appropriate age for this surgery, while 12 percent thought they would have been better off without it.
Bria Brown-King as an infant.Courtesy Bria Brown-King
Given these complexities, doctors and advocates have argued over whether children with CAH should be exempt from potential laws and policies that protect them from early cosmetic surgery. This was the case last year in California, when lawmakers, advocates and physician groups sparred over whether a bill, which would ban unnecessary surgeries on children with genital differences before age 6, was too broad. The bill, which was strongly opposed by the California Medical Association and Societies for Pediatric Urology, a group that represents the doctors who treat these patients, did not pass.
“The right answer right now isn’t clear,” Dr. Beth Drzewiecki, chief of pediatric urology at Tufts Children’s Hospital in Boston, said. “However, a blanket ban on surgery will not accurately support the views and voices of all of those that have variations in sex development.”
While Lurie Children’s Hospital has ended early medically unnecessary surgeries, it is considering an exemption for children with CAH, who experts say make up a majority of those who undergo feminizing surgeries. In an email, a spokeswoman for the hospital said the surgeries “will not be performed on CAH patients until we have evaluated the best practices and ethics and have released a white paper or report on the topic.”
The risks of ‘gender-normalizing surgeries’
There are no laws in the U.S. that regulate medically unnecessary gential surgeries for intersex children, Meanwhile, the current standard of care “remains an interdisciplinary team approach informed by parents’ wishes,” according to the AMA Journal of Ethics.
Taking this approach, more hospitals are hiring teams of surgeons, psychologists, social workers and genetic experts who work together to better understand a baby’s unique specific intersex trait, a process that can take weeks or even months, according to experts who work with these children. And doctors today are less likely to rush to assign a gender, though this may not always be the case.
“We still make recommendations for what gender we think the child is best going to feel, and we work that way,” Stred said. In cases where it is difficult to assign a sex, she said some doctors may recommend giving the child a gender-neutral name in case the child later disagrees with what sex they have been assigned.
Surgical techniques have improved greatly since the 1950s, with a better understanding of how to preserve sensitive nerves and tissue, according to Drzewiecki. She also said more surgeons today are giving parents options, rather than recommending surgery as a default solution.
“It’s really, I think, important to affirm to the families that their child is going to be OK with or without surgery,” she said, adding that “the most important thing is having transparency about what the risks are, and what the long-term risk over time will be, as well.”
One risk for those with CAH is stenosis, a condition in which surgically altered vaginal openings — performed in order to separate the urethra from the vaginal canal, which are typically fused in these children — can narrow over time, according to doctors. While the procedure is done to create a more typical vagina, doctors say it may be medically necessary to prevent urinary tract infections in some children, though the need for this is debated. A contentious way to prevent stenosis has been for parents or doctors to periodically insert a dilator in the opening to maintain it, though experts say this is usually traumatizing for children and, as such, is rarely done anymore.
Stenosis can lead to issues with menstruation and sex later in life, and may require additional surgery to fix, according to Dr. Frances Grimstad, a pediatric and adolescent gynecologist at Boston Children’s Hospital, who has training in these surgical repairs. And in general, she said, any early surgery performed on a child’s genitals is “playing a guessing game” as to what they will need or want in the future. Overall success rates of early surgeries are hard to pinpoint, she added, since health and insurance databases don’t accurately track them, and medical research tends to focus only on early outcomes.
“Surgeons who are doing these surgeries typically don’t follow their patients into their early 20s,” she said.
Brown-King said they developed urinary tract infections both before and after surgery and had to get additional surgery at age 19 to fix scar tissue.
“Surgery doesn’t fix everything,” they said. “I think that that’s kind of a narrative that sometimes doctors like to paint, that once you have surgery, things will be great. But that’s not necessarily the case.”
Surgery can also lead to mental health problems later in life, especially for those whose parents kept it a secret from them, according to Dr. Katharine Dalke, a psychiatrist at Penn State Health who specializes in LGBTQ and intersex populations. For many, she said, this sent a message that there was something “fundamentally wrong” with who they are, and that they “weren’t lovable otherwise.”
Parents struggle with surgery decisions
While some medical professionals are beginning to take a more nuanced and affirming approach to intersex care, the decision to perform early surgery remains in the hands of parents, who vary widely in their attitudes toward sex and gender. And many struggle to cope with the challenges of raising a child with a gential difference in a world that wants to know, “Is your baby a boy or a girl?” Under this pressure, parents may feel that “doing nothing equals doing harm,” according to Stred.
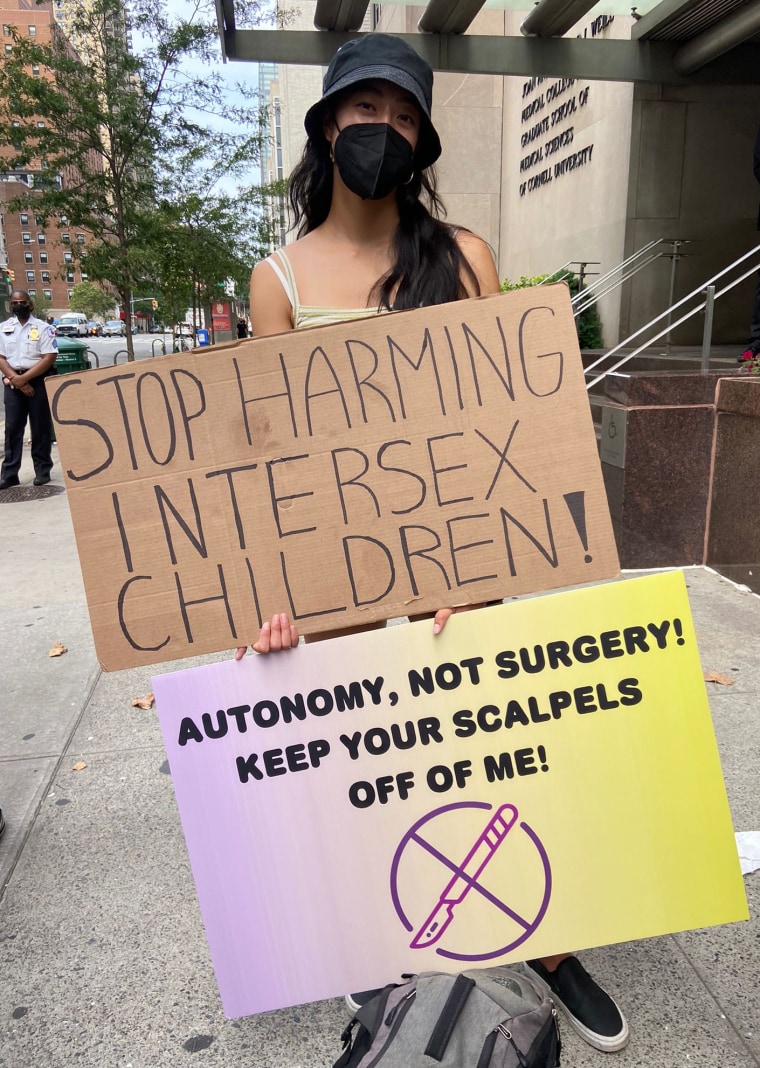
A protester outside Weill Cornell Medical Center in New York on Aug. 7.Casey Orozco-Poore
However, doctors say more parents are deciding to delay surgery, though it’s unclear how common this is. Those who make this choice often navigate a difficult journey alone, with few support groups or resources to guide them.
NBC News spoke to the father of a 6-year-old girl with CAH, who requested that his name not be published to protect his daughter’s privacy. So far, she identifies as a girl, though she is gender-nonconforming, and has had no issues with urinary tract infections, he said.
While he wants her to have “autonomy in determining her own identity,” he also said he worries she will resent him for not getting the surgery. He said he would let her get the surgery when she is old enough to decide.
“My fear is that she will want to do the surgery because of social pressure or peer pressure, and doing something simply to conform or avoid being different, I would have a harder time supporting,” he explained.
Dalke said that helping kids with genital differences begins with understanding “there’s nothing inherently pathological about” them, and that with help from parents and mental health providers, they can learn how to cope with bullying and even thrive.
For this reason, intersex advocates have fought for better education and psychological support for parents, and some lawmakers have begun to listen. That was the case this year when the New York City Council passed a bill that requires the city’s health department to provide intersex-inclusive education to parents and doctors.
There are hospitals that already provide psychological counseling for parents of intersex children, and some parents still struggle in spite of it. Recalling one mother who body-shamed her child during visits, Drzewiecki said children raised in nonaffirming environments are susceptible to psychological harm. And while it’s ideal to raise these children in an affirming way, she said, it’s “unrealistic” to expect that of “everybody in our society right now.”
As for Brown-King, they said surgery did not spare them from bullying, nor are they “worried about finding love” over the way they look. When asked whether those with CAH should be excluded from surgical delays, they posed a different question: “Why aren’t we having conversations with our children about the different ways to have a body?”
“There’s no such thing as having a clitoris that’s too large,” Brown-King said. “In the same way that penises come in all different shapes and sizes, so do clitorises. Why can’t we start to push that narrative instead?”