An appellate court deciding Hobby Lobby violated Illinois anti-discrimination law by denying a transgender employee access to the women’s restroom could have nationwide implications, experts say.
Meggan Sommerville, a trans woman who has worked at a Hobby Lobby location in Aurora for more than 20 years, has been denied access to the store’s women’s room since transitioning at work in 2010. As a result, she has had anxiety and recurring nightmares and has been forced to limit her fluid intake, according to filings.
On Friday, the Illinois 2nd District Appellate Court upheld a lower court decision that determined the crafts chain violated the Illinois Human Rights Act both as an employer and as a place of public accommodation.
“Sommerville is female, just like the women who are permitted to use the women’s bathroom,” the three-judge panel said in its decision. “The only reason that Sommerville is barred from using the women’s bathroom is that she is a transgender woman.”
The ruling is one of first impression, meaning it presents a legal issue that has never been decided in the court’s jurisdiction.
“They stuck to the law,” Sommerville, 51, told Forbes. “This is a precedent-setting case in Illinois, because the Human Rights Act has never been tested in this way in Illinois, and actually in the country.”
Jim Bennett, director of the Illinois Department of Human Rights, said the decision underscored that trans people in the state “have strong protection from discrimination.”
“Ms. Sommerville’s experience of discrimination is certainly not unique, as too many of our transgender friends and neighbors continue to face acts of discrimination and hate,” Bennett said in a statement. “With this decision, the IDHR has been given a clear path to enforce the Commission’s orders concerning the rights of trans persons.”
Jacob Meister, who represented Sommerville, went further, telling Bloomberg Law the decision had national implications and will “start the process of courts around the country addressing the issue of bathroom access.”
Camilla Taylor, litigation director for the LGBTQ legal advocacy group Lambda Legal, agrees the ruling could have a broad impact in a variety of areas and jurisdictions.
“I think other states will generally be able cite this ruling, because of how sweeping it is,” Taylor said. “This is not limited to employment. This is the public policy of the state of Illinois. The court went out of its way to knock down every justification for treating trans people differently in public. It made it clear there’s no justification.”
While the Supreme Court’s 2020 decision in Bostock v. Clayton County, Georgia, determined discrimination based on sex includes sexual orientation and gender identity, it didn’t address access to sex-segregated facilities, services or sports teams.
“You can’t argue it’s not sex discrimination to deny someone access to a bathroom or a locker room,” Taylor said.
Not only could the ruling be used by opponents of so-called bathroom bills, she added, it could be relevant to the legal fight against legislation prohibiting transgender girls from playing on female sports teams.
“It will have big ramifications in all kinds of aspects of life — in education, in business, in gyms and sports,” Taylor said. “It’s indicative of applying nondiscrimination principles to sex-segregated areas. It makes clear that gender identity determines sex.”
Hobby Lobby could appeal the ruling to the Illinois Supreme Court and theoretically take it all the way to the U.S. Supreme Court. Attorney Whitman Brisky, who represented the company, did not immediately reply to a request for comment.
The 2021 legislative session has set a record for anti-transgender bills, according the Human Rights Campaign, an LGBTQ advocacy group: Nearly 70 measures were introduced in at least 30 states that would prohibit trans youth from participating in sports consistent with their gender identity, and at least 15 bills were introduced that would bar trans people from accessing the restrooms or locker rooms that align with their gender identity.
The judicial branch, however, has been more supportive: In addition to Bostock, the Supreme Court in June declined to review a 4th U.S. Circuit Court of Appeals decision that ruled transgender student Gavin Grimm had a constitutional right to use the boys’ restroom at his Virginia school.
The lower court ruled that policies barring transgender students from restrooms that match their gender identity violate the equal protection clause of the 14th Amendment and Title IX of the Education Amendments of 1972.
For three years, Jesse Brace avoided getting care for their seizures after they experienced discrimination at an emergency room near their home in Lawrence, Kansas, in 2017.
They said they told the staff that they are transgender and nonbinary, that their name is different from their legal name and that they use gender-neutral pronouns.
“They refused to even so much as acknowledge this information, and not only did they not use [my pronouns], but they also sent me home without treating me for what I went in for,” said Brace, 25.
When they tried to get care elsewhere after that, they said, they had similar experiences, so they avoided care entirely.
Jesse Brace. Courtesy / Jesse Brace
In 2018, they began having seizures every day, so they started living in their car outside the Amazon facility where they were an assistant operations manager, because they couldn’t drive themself to work anymore.
In November 2018, they lost their job. “I lost my car soon after and ended up on the streets in the winter,” they said. “I was having hundreds [of seizures] a day and wasn’t even leaving where I was laying.”
They were homeless, living out of their car or on the streets, for over three years.
Brace’s experience in the ER — and the impact that health care discrimination had on their life — is something many trans people face and fear when they try to get care, according to a report released Wednesday by the Center for American Progress, or CAP, a liberal think tank.
Discrimination, among other factors, prevents trans people from seeking necessary care, which leads to health disparities that can affect many other areas of their lives, the report found.
The authors outline a road map of solutions, including legislative protections for LGBTQ people and better competency training for medical providers.
“The onus should not be on individuals,” said one of the report’s authors, Sharita Gruberg, vice president of the center’s LGBTQ Research and Communications Project. “It really should be on these institutions to do the right thing, and the resources and guidance is out there.”
Forgoing routine care after trauma
CAP’s report found that nearly half of transgender people — and 68 percent of transgender people of color — reported having experienced mistreatment at the hands of a medical provider, including refusal of care and verbal or physical abuse, in the year before the survey, which took place in June 2020.
Discrimination can then prevent people from seeking future care, the survey found: 28 percent of transgender people, including 22 percent of transgender people of color, reported having postponed or not gotten necessary medical care for fear of discrimination.
Brace got another job in May 2019, but they said they weren’t able to get consistent care again until May of this year. They said doctors in the area repeatedly told them that they were unable to take on new patients. It wasn’t until Brace was referred to a doctor who has a transgender child that they were finally able to obtain a primary care physician.
“I get panic attacks just making appointments,” they said. “I have no support whatsoever. Unfortunately, all health care around here is like this. There is no support for trans people, and so most avoid seeking care.”
Dallas Ducar, a psychiatric nurse practitioner, opened Transhealth Northampton, a trans-led organization that provides health care to trans and gender diverse patients in western Massachusetts, in May. Ducar said that as a health care provider and a trans woman, she knows there’s a dearth of affirming care for trans people across the country.
The Transhealth Northampton team. Courtesy / Dallas Ducar
She said many of Transhealth’s patients have gone without medical care for long periods of time. A patient who came in a couple of months ago had abnormal vital signs and had to be quickly taken to an emergency room because they were so sick, she added.
“It’s unfortunately not uncommon to see people who have experienced such high levels of discrimination and then forgo the routine visits, then perhaps even forgo an urgent care visit, which then turns into an emergency care visit,” she said.
The CAP report said harassment and discrimination “contribute to high rates of stress,” and — along with social determinants of health — make trans people “more likely to experience poor health outcomes.”
People will read about health disparities among trans people “and just think of that as something that, horribly, is associated with just like being trans, but actually a lot of these experiences have to do with being trans in a world that is constantly oppressing you and where you’re experiencing discrimination both interpersonally but also institutionally and in these broader systems,” said one of the report’s authors, Caroline Medina, a policy analyst at CAP.
The report cites the 2019 Behavioral Risk Factor Surveillance System data collected by the Centers for Disease Control and Prevention, which found that trans people were more than twice as likely as cisgender adults to be told they had depressive disorders.
Fifty-four percent also reported poor physical health at least one day in the previous month, compared to 36 percent of cisgender respondents, according to the CDC data. Trans people also have an increased likelihood of having asthma and developing cardiovascular disease, according to the CAP report.
The Covid-19 pandemic has also aggravated the health disparities trans people face: 1 in 3 reported having had suicidal thoughts during the pandemic, and 1 in 2 reported that their access to gender-affirming health care was curtailed significantly during the pandemic.
Ducar said barriers to care, particularly gender-affirming care like hormones, is “really, really harmful, and they add to the layers of discrimination that exists within the trans community.”
“On the mental health side, we are seeing folks with really complex issues — tons and tons of trauma — that’s coming to our doorstep,” she said. “We’re just seeing a lot of not only trauma, but complex PTSD specifically. These are people that have just been consistently burdened with the symptoms of PTSD, trauma just recurring. It’s really been terrible.”
A lack of cultural competency
When trans people do try to seek health care, they can face discrimination or outright refusal of care, as CAP found. But even when they don’t experience discrimination, they are likely to see providers who don’t have the cultural competency to provide them with affirming care.
CAP’s survey last year found that 1 in 3 transgender people reported having had to teach their doctors about transgender people to get appropriate care, and 15 percent reported having been asked “invasive or unnecessary questions about being transgender” not related to their reasons for visiting.
The report cited a 2018 brief from the Kaiser Family Foundation that found that more than half of medical school curriculums lack information about unique health issues the LGBTQ community faces and don’t cover treatment beyond HIV prevention and care, “likely contributing to transgender people’s inability to access affirming care,” CAP wrote.
Alex Petrovnia, 24, a writer and scientific researcher living in central Pennsylvania, said that last fall, he had to report a primary care physician after a negative experience.
He was worried about how testosterone would affect a joint problem he was having, and he asked the doctor, who was still a medical resident, whether there was a form of physical therapy to help the problem. After a tense exchange, he said, the doctor told him, “I don’t know anything about this, because I’ve never had a patient like you.”
“I was trying to keep this interaction peaceable, and I replied with: ‘Yeah, I know. It’s really unfortunate that you’re not taught anything about trans people in medical school, and it’s just not a very well-known issue,’” he said. “And she looked me right in the eyes and she said: ‘I don’t think it’s that important. There aren’t many of you.’”
When he left, he tweeted about the visit so other trans people in the area would know not to see that doctor.
The medical practice reached out to him a few days later and asked what it could do better, Petrovnia said. When he returned to see a new, supportive primary care physician, “they told me that they sent the resident back to trans-inclusivity training and that they had instituted that for all of their residents going forward,” he said. “So that was very positive. … Being the squeaky wheel really actually made an impact and actually improved the situation theoretically for others.”
Petrovnia acknowledged that not everyone is able or willing to spark such teachable moments.
Mel Groves, 25, visited a primary care office in Montgomery, Alabama, in January when he had a cough, fever and lower body pains. When he was taken back for a full-body CT scan, he said, he had a decent conversation with the attendant who was pushing his chair. Groves said that when the procedure was over, however, the attendant’s tone changed. The attendant had apparently seen Groves’ chart and made a comment about his genitals, Groves said.
Mel Groves, a farmer from Jackson, Mississippi.Courtesy / Mel Groves
“I was taken aback,” he said. “It was shocking, to say the least.”
Groves said that he wanted to report it but that he was feeling too ill and overwhelmed, as he was working in the area temporarily. “I knew that that’s what I should have done, but at the time, I had a lot of stuff going on,” he said.
The health care system that oversees the primary care office where Groves was treated could not confirm his story, citing patient confidentiality.
‘The role falls on society’
CAP’s report outlines a number of policy recommendations that the authors said would help address health care discrimination against trans people.
One in particular is among the most pressing, the authors said: They recommend that the federal government create a rule to strengthen Section 1557 of the Affordable Care Act, which prohibits discrimination on the basis of sex and has protected trans people from discrimination in federally funded health care facilities.
“The protections in Section 1557 are so critical but are also a floor that we need to firmly establish and strengthen,” said Gruberg of CAP. She said it was great that the Department of Health and Human Services’ Office of Civil Rights had announced that it would enforceSection 1557 to cover sexual orientation and gender identity, “but we’re also very worried about what that looks like, how strong these protections are going to be and the potential for religious exemptions to undermine them.”
U.S. District Judge Reed O’Connor issued a permanent injunction last week against the nondiscrimination protections in the Affordable Care Act, ruling in favor of religious health care providers who said the rules would force them to perform abortions or provide gender-affirming treatment against their religious beliefs. While Gruberg expects the decision to be overturned, she said “that threat is still there.”
The report’s authors also recommended that Congress and state and local governments increase funding for LGBTQ community health centers, which often fill the health care gaps that trans people face.
Groves was connected with an affirming primary care physician through the Knights and Orchids Society, a grassroots organization in Selma, Alabama, led by Black trans people. He drives about 4½ hours from his home in Jackson, Mississippi, to Auburn, Alabama, when he needs care.
Although groups like the Knights and Orchids Society have provided what Groves described as “life-changing” support, he said it’s ultimately up to the medical system and society to address pervasive issues like discrimination.
“We’ve always been here,” he said. “So I think that now the role falls on society and the medical professionals to educate themselves more. If that means more fellowships, more trainings, more professional development … I feel like that is single-handedly the best thing that we can do to foster better health care for trans people, is helping people to understand how to be inclusive, and then going forward from there.”
Some LGBTQ OnlyFans creators say the changes could jeopardize one of their primary sources of income during the Covid-19 pandemic.
Many sex workers, such as Stacey Monroe, 27, have been using OnlyFans to create sexually explicit video content and photos during the pandemic because they can’t see clients in person safely.
Monroe said she left her career in health care to focus on advocating for transgender rights after she faced discrimination from multiple past employers because she’s a trans woman. “However, being an activist is really a volunteer job, so there was no pay,” she said. In 2018, sex work “helped me and my sister get through our housing crisis and so many other things. It became our form of survival.”
Stacey Monroe said OnlyFans’ policy change could jeopardize 40 to 50 percent of her income.Pedro Morales
Sex work has helped them maintain stability without facing employment discrimination. Now, Monroe said, 40 percent to 50 percent of her income comes from OnlyFans subscriptions.
“If I’m not able to see customers in person, then I do have to try to make OnlyFans content and things like that, so now I’m kind of in limbo trying to figure out what am I going to do on October 1 and trying to see if there’s a loophole or anything to work around the policy,” she said.
OnlyFans’ new policy will allow creators to continue to post nude photos as long as they are consistent with the platform’s acceptable use policy, but it will prohibit “the posting of any content containing sexually-explicit conduct,” a spokesperson said in a statement.
“In order to ensure the long-term sustainability of the platform, and to continue to host an inclusive community of creators and fans, we must evolve our content guidelines,” the statement says. “These changes are to comply with the requests of our banking partners and payout providers. We will be sharing more details in the coming days and we will actively support and guide our creators through this change in content guidelines.” https://iframe.nbcnews.com/U5CK7jN?app=1
The spokesperson declined to comment on when a nude photo could be considered sexually explicit or who would screen content and decide whether it violates the policy.
OnlyFans has provided a legal avenue for people to participate in sex work. Subscribers pay monthly or yearly fees in exchange for pornographic content or one-on-one live video chats with creators, among other content.
Transgender people are more likely than the general population to participate in sex work for a variety of reasons. As a result, many LGBTQ sex workers said the community is disproportionately — and negatively — affected by OnlyFans’ policy change.
A form of survival for trans people
In 2018, Monroe and her sister, who is also trans, were facing homelessness.
“We were sleeping in our car. We had contemplated suicide,” she said. “We just really didn’t have any options. We were going to homeless shelters, and they were telling us that we were not allowed there because we were trans and they didn’t know how to accommodate us.”
With support from their community, they were able to get back on their feet, and sex work has since helped them survive, Monroe said.
Monroe’s experiences of job discrimination and homelessness are common among trans people — including trans people who participate in sex work.
A 2015 survey found that 10.8 percent of trans respondents had participated in some form of sex work, with rates the highest among Black trans respondents (39.9 percent) and Hispanic or Latino respondents (33.2 percent). Transfeminine respondents were twice as likely to participate in the sex trade, at 13.1 percent, compared to transmasculine respondents, at 7.1 percent.
The survey found that more than two-thirds (69.3 percent) of trans sex workers reported having experienced adverse job outcomes in the traditional workforce, such as being denied jobs or promotions or being fired because of their gender identity or expression. In addition, those who lost jobs because of anti-trans bias were about 2 ½ times as likely to engage in the sex trade (19.9 percent vs. 7.7 percent of respondents who didn’t lose jobs because of anti-trans bias).
The OnlyFans log in page on a laptop in New York, on June 17, 2021.Gabby Jones / Bloomberg via Getty Images file
Monroe said sex work is a form of survival for many trans people, because it allows them to earn enough money to get safe housing.
OnlyFans has provided a safer — and legal — outlet for people to engage in sex work, especially trans people, who often face violence. At least 34 trans and gender-nonconforming people have been killed this year. Most of them were Black trans women, according to the Human Rights Campaign, and some of them were also sex workers, according to memorial posts and local reports.
Monroe said some trans people use OnlyFans to pay their bills and get health care, such as hormones, during the pandemic. As a result, the policy change could affect trans creators in many ways if it’s their primary form of income.
“A lot of us have found safety in not having to see customers in person, one, because of Covid-19, and two, because of the violence against trans people and how it’s been increasingly just getting worse and worse over the years,” she said. “It’s horrible. So we are going to be facing more safety issues, more issues with housing, medical, trying to just survive in general.”
Jeopardizing stability, safe space
Z, 27, said OnlyFans has provided them with a stable and safe source of income during the pandemic. They asked to go by their initial because they hope to get a job outside sex work in the future.
They are immunocompromised and disabled and were unable to leave their home at all before a Covid-19 vaccine was available.
They began using OnlyFans in November to sell lewd photos. They incorporated their mobility devices into shoots and described themself as openly queer. In their first month using the platform, they said, they doubled their average monthly income and were able to hire a personal care attendant to help them with their physical therapy exercises and daily activities, such as washing their hair and prepping meals.
They said the OnlyFans policy change will affect them because they don’t have an audience for the type of content that OnlyFans now says is within its terms of service, though they noted that they won’t be as affected as other creators who do more video content.
“I think that when you are specifically advertising sex worker services and then those services are no longer what you’re able to provide, nobody’s going to be there for that,” they said. “I don’t foresee getting a lot of income from people who would just want to see pictures of my smiling face every day.”
OnlyFans no longer makes up the bulk of Z’s income, but they said it does provide them with a few hundred dollars a month, which can cover their physical therapy, medication or groceries.
OnlyFans is used primarily by sex workers who sell pornographic content, but creator GothyKitten, 33, who asked to go by their username on the platform, used it to share time-lapse photos of their surgery site after they had gender-affirming surgery. They uploaded a year’s worth of images in late December.
“A couple folks have said that it really helped them with considering surgery, and everyone who asked for it said they couldn’t find any other resources as detailed,” they said. OnlyFans’ new acceptable use policy will ban “any exhibition of the anus or genitals of any person which is extreme or offensive,” and it doesn’t define “extreme” or “offensive,” leaving GothyKitten uncertain whether their content will be removed.
For now, they’ve created an account on AdmireMe.vip, a site that posted a message of support to sex workers after OnlyFans announced its policy change.https://iframe.nbcnews.com/468GgCb?app=1
For some LGBTQ OnlyFans creators, like Jack Mackenroth, 52, the platform’s new policy is disappointing but not necessarily negative. Mackenroth created an OnlyFans account to share gay pornographic content shortly after the site started in 2016.
He said that the site isn’t user friendly and that there are better platforms that were created by sex workers, like JustFor.fans, which also shared a message about OnlyFans’ policy.https://iframe.nbcnews.com/h8cOaI7?app=1
Sex workers made OnlyFans “what they are,” Mackenroth said, and now it won’t fight for the creators who helped build the site. “They seem to be fair-weather friends, and I don’t need those,” he said.
He encouraged OnlyFans creators to move their content to other platforms and diversify their sources of income.
Jack Mackenroth attends “The Imitation Game” NYC premiere on Nov. 17, 2014. Jim Spellman / WireImage – Getty Images file
LaLa Zannell, the Trans Justice Campaign manager at the American Civil Liberties Union, said being able to change platforms is a privilege not all sex workers have.
“A person who is navigating just surviving, navigating transphobia, xenophobia and homelessness doesn’t have time to create a whole new following on a new platform,” she said.
A number of websites that sex workers used, such as Backpage and Tumblr, were also shut down or changed their policies in ways that negatively affected sex workers, she said, in part because of policy changes by financial institutions that process their payments.
OnlyFans and similar sites have also faced pressure from conservative representatives and advocacy groups. Rep. Paul Gosar, R-Ariz., applauded the policy change, calling it “a remedy to child exploitation” in a tweet last week.
Gosar wrote a letter to the attorney general about a week before the site announced its policy change requesting an investigation into OnlyFans “for promoting, and profiting from, online prostitution.” The bipartisan letter was signed by more than 100 other members of Congress.
Gosar wrote on Twitter that the Justice Department had found that minors were getting through OnlyFans’ vetting process, which requires creators to have bank accounts, government IDs and face scans to ensure that their faces match the provided ID.
The Justice Department did not immediately respond to NBC News’ request for comment.https://iframe.nbcnews.com/48BjpYS?app=1
Zannell said banning pornographic content from platforms isn’t a solution, because it will just move to new platforms. But users’ constantly changing platforms isn’t, either, she said. She added that she’d like to have a sit-down with banking institutions, as well as anti-pornography and anti-sex-trafficking groups — which she said are among those pressuring banking institutions to clamp down on sites like OnlyFans — to “actually have a real conversation and carve out a real goal where all parties online can be on neutral ground, because sex work is real work.”
Tony Christon-Walker was determined to set up an HIV prevention clinic in Birmingham, Alabama, that would succeed where others have long struggled to combat the scourge of the virus among his fellow queer Black men.
The director of prevention and community partnerships at the nonprofit AIDS Alabama, he spent much of 2019 hiring a clinic staff composed of people of color. They were trained to provide the kind of affirming care that, he said, “reflects our culture,” and that would encourage local men at risk of HIV to keep coming back.
Even facing the headwinds of the Covid-19 pandemic, the fledgling clinic, which specializes in prescribing the HIV prevention pill known as PrEP, for pre-exposure prophylaxis, made steady progress in realizing his vision.
But now clinics like this that provide vital HIV prevention services to disadvantaged populations are facing a dire — and for some of these nonprofit groups, even existential — financial crisis driven by the vagaries of an arcane federal law governing prescription drug discounts.
These safety net clinics are set to lose well over $100 million in annual HIV prevention funds due in part to a recent decision by the pharmaceutical giant Gilead Sciences to cut off what has become an increasingly valuable revenue stream supporting these organizations in their grassroots efforts to prevent the virus’s spread. The consequences are expected to be most devastating to clinics in the South, due to the region’s disproportionately large uninsured population and the fact that half of HIV transmissions in the United States occur in those states.
The imminent funding loss threatens to substantially compromise an ambitious plan the federal government launched last year to end the nation’s HIV epidemic by 2030. People of color will likely bear the brunt of the impact — at a time when the public health sector is striving to mitigate racial disparities, not see them worsen.
“This will shut us down,” said Christon-Walker, of how Gilead’s policy change will affect AIDS Alabama’s PrEP clinic. Losing the funds, he said, will “destroy our program and totally inhibit our ability to see uninsured clients, which make up the bulk of our business.”
Dependence on a ‘patchwork solution’
The financial morass centers around a 1992 federal drug pricing law called 340B. The law grants clinics that care for a disproportionate number of uninsured and low-income individuals the right to purchase pharmaceuticals at steep discounts through their in-house or contracted pharmacies. Public and private insurers typically reimburse 340B-designated clinics’ pharmacies at a dollar amount close to a prescribed drug’s list price; and in a unique setup that Gilead recently decided to end, citing ballooning costs, the California-based company has long engaged in a similar reimbursement process when providing free antiretrovirals for HIV treatment or prevention to uninsured people. Such transactions yield surplus cash — known as the “340B spread” — that these organizations spend on their services.
For expensive brand-name drugs, the 340B spread can be quite a substantial sum. By contrast, when these clinics prescribe a cheaper generic medication, the difference between the price they pay and the price at which they are reimbursed is often relatively minimal; so the prescription generates little revenue.
The Food and Drug Administration approved Gilead’s antiretroviral Truvada for use as HIV prevention in 2012. David Paul Morris / Bloomberg via Getty Images
Consequently, even as the Biden administration seeks to drive downthe cost of pharmaceuticals, the little-publicized 340B pricing law conversely — and perversely — causes many health care facilities serving low-income individuals to depend on drug prices for all kinds of health conditions remaining high to support their bottom lines.
Tim Horn, director of health care access at the HIV advocacy group NASTAD, said the 340B funding system is a “patchwork solution” to the woeful lack of investment in the nation’s medical and public health safety net, and one that amounts to “a house of cards.”
Because of the high price of antiretrovirals used to treat and prevent HIV, the 340B spread funnels hundreds of millions of dollars annually into HIV-focused safety net clinics that serve the low-income, uninsured and nonwhite populations that are disproportionately impacted by the virus. The additional funds allow these clinics to provide extra services, such as transportation assistance or case management.
In the coming years, high-quality HIV treatment regimens will increasingly go off patent. This is good news for the nation’s overall health care bill, and state Medicaid budgets in particular. But as cheaper generic antiretrovirals enter the market, safety net clinics treating people with HIV will sustain a progressive and potentially devastating loss of their 340B revenue.
Currently, however, the most pressing 340B-related financial concern in the national HIV arena revolves around revenue tied to the historically pricey PrEP.
The Food and Drug Administration approved Gilead’s antiretroviral Truvada for use as HIV prevention in 2012. PrEP’s popularity has soaredin recent years, and the Centers for Disease Control and Prevention recently estimated that about 285,000 people — overwhelmingly white gay and bisexual men — were taking it by 2019. The federal agency credits PrEP with helping drive the modest 8 percent decrease, from 37,800 to 34,800 cases, in estimated annual HIV transmissions in the U.S. between 2015 and 2019.
But PrEP’s use has remained disappointingly limited among Black and Latino men who have sex with men, who comprised a respective 25 percent and 21 percent of the 36,800 new HIV diagnoses in 2019, according to the CDC. These are disparities that 340B clinics have worked hard, and are uniquely positioned, to address.
Daniel O’Day, CEO of Gilead Sciences, testifies during a hearing on why Truvada is so expensive, on May, 16, 2019 in Washington.Bill O’Leary / The Washington Post via Getty Images
In recent years, the activist group PrEP4All has campaigned against Truvada’s high price, which Gilead has raised from $1,160 per month in 2012 to $1,842 today. The activists have claimed that Truvada’s cost has been the predominant factor limiting PrEP access in the nation — a claim echoed by Dr. Rochelle Walensky, now the CDC director, during a May 2019 congressional hearing held over Gilead’s high list price for PrEP.
And yet, PrEP is widely covered by insurance, with federal guidelines requiring that almost all private plans, as well as state Medicaid programs expanded under the Affordable Care Act, cover it with no cost-sharing. Gilead also providesfree PrEP to uninsured people.
Moreover, the high price of Truvada, and now also Descovy — an updated version of Truvada that the FDA approved as the second available form of PrEP in 2019 — has actually been a financial godsend to the 340B clinics that serve the very populations among whom HIV transmission is the highest.
According to Horn, the 340B spread for a single prescription for Truvada or Descovy amounts to about $1,200 to $1,600 monthly, or $14,400 to $19,200 annually. Clinics have been able to use this windfall to subsidize for their uninsured PrEP patients the quarterly clinic visits and laboratory tests that are required to maintain the prescription and that are not covered by Gilead’s patient assistance program.
Such funds have also been channeled into paying 340B clinics’ facility and technology costs and to pay for patient navigators, safe sex counselors, outreach workers, condoms, advertising, patient transportation, sexually transmitted infection screening and treatment, and opioid use disorder treatment. And in some cases, this money covers other medications for uninsured people, including the initial few months of HIV treatment before the federal Ryan White HIV/AIDS Program kicks in and picks up the tab.
Now, much of the 340B spread tied to PrEP is poised to vanish, potentially hobbling the services that help keep the HIV epidemic in check. Many uninsured people are expected to lose access to PrEP because of an inability to pay for their clinic visits and lab tests.
“It’s going to put a lot of our programs in serious harm’s way at best,” Jim Pickett, senior director of prevention advocacy and gay men’s health at AIDS Foundation Chicago said. “Some of them will be decimated and destroyed.”
Laboratory technician Brady Robles draws blood from a patient at the Kind Clinic in Austin, Texas. Kind Clinic
HIV advocates worry that this funding crisis will only exacerbate the racial disparities that have long characterized the nation’s epidemic.
“HIV has a disproportionate impact on Black and brown communities, especially here in Texas. I really fear that we will have more Black and Latinx people acquiring HIV if other funding sources aren’t in place,” Christopher Hamilton, CEO of Texas Health Action, an HIV- and LGBTQ-focused nonprofit health care provider, said as he echoed a concern shared among his colleagues across the country.
A ‘peculiar’ and ‘unsustainable’ system
After Gilead announced in early April that it would change its patient assistance program reimbursement policy starting in October, an outcry followed, prompting the companyto move the cut-off to January 2022.
Also in April, multiple generic versions of Truvada entered the market for the first time. Some have a list price as low as $30 per month, posing a major threat to Gilead’s highly profitable PrEP sales.
This price plunge heralds a second oncoming financial crisis for 340B organizations. Insurers are already starting to push people with PrEP prescriptions off of Descovy or the brand-name Truvada and onto the cheap generic drug. Should this shift persist, 340B revenue tied to insured people receiving PrEP will steadily deplete.
In recent years, the activist group PrEP4All has campaigned against Truvada’s high price, which Gilead has raised from $1,160 per month in 2012 to $1,842 today. BSIP / Universal Images Group via Getty
Determining how much money is at stake with the 340B spread tied to PrEP — even Gilead says it does not know the true sum — largely requires querying each clinic individually. The Health Resources and Services Administration recently ascertained from 195 health centerssplitting a $54 million HIV-prevention grant from the agency that in 2020, these clinics prescribed PrEP to 63,000 people — up from 20,000 the previous year. According to the agency, which had no comment for this article, 96 percent of these centers participate in the 340B program. And while it is unknown what percentage of these PrEP recipients are uninsured, overall about a quarter of HRSA-funded health centers’ patients lack health insurance.
NBC News asked nearly 120 HIV prevention-focused 340B clinics for their PrEP-patient figures. The vast majority were unresponsive or refused to share their data. Many said they were wary of alienating Gilead, given the clinics’ further dependency on charitable grants from the company, which is the dominant manufacturer of HIV-treatment pharmaceuticals.
Nevertheless, NBC News was able to tally that at the very least, some 7,000 uninsured 340B clinic patients nationwide are receiving free PrEP from Gilead’s patient assistance program monthly. This modest figure alone translates to a pending minimum loss in 340B-spread revenue to such clinics of $100 million annually starting in January. Given the low response rate to queries — data on roughly 3,000 of these patients came from publicly available information concerning California, and the remainder came from just 24 clinics elsewhere — and given the implication of the HRSA figures, the true dollar figure is likely considerably higher.
“It is peculiar that all of these organizations have been able to get all this funding for receiving a free drug,” said Carl Schmid, executive director at HIV + Hepatitis Policy Institute in Washington, D.C. “But that’s the system that we have been living with, and people have been counting on that for years.”
During an April 8 call between HIV advocates and Gilead to discuss the impending financial changes, Eric Leue, vice president of prevention services at the HIV-prevention clinic Friends for Life in Memphis, Tennessee, was clearly distraught as he pleaded with company representatives to reconsider their change in policy. Noting that Memphis has one of the nation’s highest HIV diagnosis rates, Leue said, Gilead’s “unconscionable”impending reimbursement cutwill force his clinic to close, and that overall, it “will set this county and our population back by at least another decade.”
Coy Stout, vice president of market access strategy at Gilead, explained in an interview that the company never intended to establish the 340B revenue stream in question. In 2004, eight years before PrEP was even approved, Gilead made a fateful decision regarding the administration of its patient assistance program. Instead of having a single contracted mail-order pharmacy send free antiretrovirals to uninsured people directly, as pharma companies typically do, Gilead decided it would reimburse the nation’s pharmacies for purchasing the company’s HIV antiretrovirals and hepatitis B antivirals. According to Stout, the intention was to make filling prescriptions convenient for uninsured patients.
Gilead did not expect pharmacies to purchase substantial quantities of the company’s antiretrovirals at 340B discount prices, because the Ryan White HIV/AIDS Program covers HIV treatment for the uninsured and underinsured.
But the U.S. government would establish no such safety net program to pay for PrEP.
So particularly in the 13 states that have not expanded Medicaid, which are concentrated in the South, there are now substantial — and ever growing — numbers of uninsured people receiving free PrEP from Gilead’s patient assistance program through 340B clinics.https://iframe.nbcnews.com/V9XOgMB?app=1
As for insured people receiving PrEP at 340B clinics, responses from the 24 clinics pointed to some 2,850 such individuals receiving brand-name Truvada and 5,900 receiving Descovy. These figures, which experts believe represent vast underestimates of actual national totals, translate to at least $125 million in annual 340B revenue that stands to diminish given insurers’ efforts to push patients onto cheap generic versions.
To put the cumulative pending loss of 340B-spread funds into context, the federal government funded the “Ending the HIV Epidemic” plan by increasing the HIV-related budget by $267 million in 2020 and by $405 million in 2021. The Biden administration’s 2022 budget request has sought to raise this additional outlay to $670 million.
HIV policy advocates like Schmid have been pushing Congress, the Health Resources and Services Administration and the CDC for increased funding to address the lost revenue tied to PrEP’s 340B spread. The CDC traditionally forbids clinics from spending agency grant money to pay for the lab tests and clinic visits for uninsured people on PrEP. However, it does allow Ending the HIV Epidemic-related grants to cover such costs.
From Gilead’s perspective, its patient assistance program is well over budget and, according to Stout, is “unsustainable.” He further stressed that the company is not able simply to turn around and donate the lost 340B spread to the impacted clinics. Under federal tax law, charitable contributions on Gilead’s part cannot be directly geared around their own commercial products.
“It makes good business sense for Gilead to change the policy,”NASTAD’s Tim Horn said, “but it’s just very, very unfortunate timing.”
Like most LGBTQ families, my partner and I didn’t become parents in the most conventional way.
In fact, for most of my life, I never considered having kids! But when my partner and I got a call asking if we’d be willing to take immediate guardianship of our niece and nephew, we agreed to do everything in our power to create a loving home for these two children.
After years of visits from social workers, inquiries from investigators trips to the courthouse, and mountains of paperwork and fees, we had the privilege of becoming a forever family through legal adoption.
If you are considering adoption, here are 7 things you should know from my personal experience:
Adoption is a story of joy…
None of us will ever forget the day that our adoption was finalized. To know that we could truthfully tell these amazing children that we would always–ALWAYS–be their parents. It was a day of pure relief.
But in addition to those big milestones – Adoption Day, kindergarten graduation, first performance as a Russian dancer in The Nutcracker – it’s really the little things that bring the most joy. The simple moments are what get to me the most. When they reach for your hand because they’re scared (and you get to tell them it’s okay to be scared). When they learn a new fact and share it with you (did you know that elephants use mud to cool themselves down). When they ask a hard question that you don’t *totally* know the answer to (how DOES an apple seed know how to grow into a tree?!).
Those opportunities to see your children grow into whole, complete humans with their own thoughts, ideas, and passions. That’s joy.
And finally, one of my absolute favorite things about being a parent is having the opportunity to share LGBTQ culture with them. Helping them build an enduring appreciation of drag. Feeling the freedom of getting to pick your own family, your own community, even your own name. All of the powerful, beautiful parts of our community– we get to pass those on to our children.
…and also one of loss
There is no way to get around the fact that your adopted children get to be in your lives because they do not get to be in the lives of their biological parents. While many adopted children will grow up to have no desire to know their biological parents, some feel a profound sense of loss or abandonment that they could not be raised by their biological parents, no matter how wonderful and caring their adoptive parents are.
It’s vitally important for adoptive parents to accept this pain in their children, to sit with it, to be empathetic, and to not take it as a personal rebuke to your parenting. Make sure that your kids have professional support throughout their childhood, and give lots of opportunities for them to share their feelings with you in a safe way.
Make sure that you have support as well, so you can process through the many feelings you may have– feelings of grief that you aren’t their biological parent or that you couldn’t have biological children. Feelings of anger towards their first family and what harmful experiences your children may have experienced while under their care. Feelings of love toward their first family for allowing you to raise their biological children.
Many complicated swirls of emotion may come up as you go on this journey, and you’ll need a place to put them all.
Parenting is not for the faint of heart
Your kid might not like you. You might not like your kid (all the time). Your kid might have severe emotional trauma. Your kid might do this annoying thing where he lies on the couch for two hours flipping a pillow over his head while the rest of you are doing dishes and vacuuming the floor and cleaning the tub.
When you become a parent, no matter how it happens, you’re not just signing up for the giggles and the tickles and the cooing sighs of a sleeping newborn. You’re also signing up for screaming babies and poopsplosions. And, after that, defiant teenagers who scream “I hate you!” and slam their door so hard the handle breaks and they have a panic attack because they can’t open their door anymore and they feel trapped. You’re signing up for their first heartbreak. For helping them deal with bullies… or BEING the bully. You’re signing up for a world of stupid, unsolicited advice and your own parents saying, “We never did that when you were a kid and you turned out fine!!!”
Despite what Instagram may tell you, parenting is not all fun and games. You’re going to mess up. You’re going to lose your temper. You’re going to yell at the lady in the supermarket who asks, “Are they REAL siblings?”
There are millions of ways to be a perfectly adequate parent. Don’t compare yourself to other parents. Be honest with your kids. Know that it’s hard for *everyone*, even the perfect families on social media.
There is no rush to start your family
When we became parents overnight in our mid-twenties, we had no idea what challenges were ahead of us. We were almost completely unprepared and had to make it all up as we went.
So any time a young LGBTQ person stands up at one of my talks and tells me that I’ve inspired them to start a family, and asks if I have advice for them, I always say the same thing: “WAIT!” Usually, the audience laughs, so I have to tell them that I am not joking.
People will tell you that you’re never really ready for parenthood. And while that’s true, there are times in life when you will be more ready! Parenting is already hard enough. Work to get your systems in place before making the leap: do your best to get your finances in order, make sure your housing is stable, and if you have a partner or partners, make sure they’re the people who truly want by your side for the next 18 years.
And above all, take the time to work on yourself and your own insecurities. If you didn’t have an ideal childhood, seek support and healing to process through it effectively so you don’t end up overcorrecting or taking your hurt out on your children. Whatever you wish your parents had worked on before they had you– you have a chance to work on those things for yourself.
Creativity, flexibility, and humility are essential
When our children first came to live with us, the eldest was nonverbal. There’s a whole section in my book in which I talk about the elaborate method I had to create so I could communicate with him – he wasn’t able to speak or share his opinions using words at all. We all had to be really creative to find solutions for their unique challenges. Many parents, especially adoptive parents, have to do the same. Build parenting solutions that work for the kids you HAVE, not the kids you wish you had.
It really does take a village
From kid supplies to legal help, our community was always there for us in ways we would never have expected. Don’t be afraid to ask for help, to invite people into your lives, to build an extended family around your actual family. Remember that most straight people have biological family around them! Grandparents help with babysitting so they can do date night, aunts and uncles help with school pick-ups so they can work late, and cousins are around for playdates and family dinners. LGBTQ people might not have that built-in support network, so we have to build it for ourselves.
Your “village” can come from outside your community as well. In fact, you can find allies anywhere – bosses may be willing to give you time off for court dates (even if that’s not covered in your PTO plan), lawyers may give you a discount on their legal fees, daycares may cut you some slack on registration costs. People want to help you form your family. Let them.
Also – sometimes you and your partner won’t see eye-to-eye. Joining a Facebook community of other parents raising their partner’s nieces and nephews (yes – there are groups this niche!) helped me keep my sanity while adjusting to the new situation. You can access vital resources and emotional support throughout your adoption journey by finding support groups for trans parents, for LGBTQ parents, for parents raising kids in open adoptions, or for whatever your specific situation is.
Love makes a family
I’ll never forget the day that we brought the kids to court for their official adoption day. Our close friends filled the courtroom and the judge, a bit taken aback by the crowd, asked, “Well who do we have here?” Our daughter Hailey, who was five at the time and didn’t understand court decorum, exclaimed, “It’s our Love Family!”
Even at that early age, she already knew that biology doesn’t dictate familial relationships. She will always be surrounded by a constellation of people who love her, support her, and will go to the ends of the earth to make sure she has what she needs to thrive in this world.
Whether your family is you and your collection of houseplants, or three parents and a gaggle of foster children – what makes a family is love.
Trystan Reese, author of How We Do Family: From Adoption to Trans Pregnancy, What We Learned about Love and LGBTQ Parenthood, launched into the public eye as “the pregnant man” in 2017 when the story of his family’s unique journey gained international media attention. He was invited to give closing performances for The Moth Mainstage in Portland, Albuquerque, and Brooklyn; a video of the Brooklyn event has garnered over 2.5 million views. As interest in his family’s story grew, Trystan partnered with many major media outlets, including CNN, NBC, People, and Buzzfeed.
Trystan is an established thought leader, educator, and speaker, focusing on diversity, equity, and inclusion. He is a professionally trained anti-racism facilitator and has been organizing with the trans community for nearly two decades. The founder of his own consulting firm, Collaborate Consulting, Trystan provides customized training solutions for individuals, organizations, and communities that are interested in social justice. He is married to his partner Biff and they live in Portland, Oregon with their three kids: Lucas, Hailey, and Leo. They are very happy.
Pope Francis invited a group of transpeople to the Vatican to be vaccinated against COVID-19 at Easter, it has been revealed.
The pontiff welcomed 50 people to the Vatican on 3 April to receive their first dose of a COVID-19 vaccine, and they returned later that month to receive their second dose, Cardinal Konrad Krajewski confirmed to theNational Catholic Reporter.
Trans people from a parish in Torvaianica were among those who travelled to the Vatican to receive vaccines after Krajewski reached out to local priest Fr Andrea Conocchia, who has been ministering to the local trans community for some time.
Others who were vaccinated as part of the initiative included volunteers, immigrants, refugees, struggling families and single parents.
Juan Carlos Cruz – a survivor of clerical sex abuse who was recently appointed to the Pontifical Commission for the Protection of Minors – told RNS that Vatican officials called Pope Francis for guidance when two buses from Torvaianica arrived as part of the vaccine initiative.
Absolutely vaccinate them!” Pope Francis said, according to Cruz. He claimed the pope went on to instruct officials to “ask for their names, ask for anything they need, but do not ask them about their sex.”
According to Conocchia, his trans parishioners reacted with “emotion” when they arrived at the Vatican to be vaccinated against COVID-19. Some of them are undocumented, meaning they are not eligible to receive vaccines under Italy’s health service.
Conocchia added: “They were moved to tears and felt remembered, having experienced once again and in a tangible way the closeness and tenderness of the pope’s charity.”
This is not the first time Pope Francis has expressed support for Italy’s trans community. In May 2020, as the world was rocked by the coronavirus pandemic, he donated funds to a group of trans sex workers who were struggling as a result of the pandemic’s economic fallout.
It was reported at the time that up to 20 trans women approached Fr Conocchia for help after their work was eradicated by COVID-19. Conocchia helped as many women as he could, but ultimately was unable to offer assistance to them all.
He subsequently wrote to Pope Francis appealing for help for his parish’s embattled trans community, and the pontiff gave the go-ahead for papal almoner Krajewski to sent money to the trans sex workers.
Catholic teaching remains firmly opposed to LGBT+ acceptance
LGBT+ Catholics will watch Pope Francis’s most recent charitable efforts with interest. The Catholic Church has historically been firmly opposed to any acceptance of queer people’s identities, and it still holds firm on its teaching that homosexuality is intrinsically disordered.
Furthermore, there was dismay among queer Catholics in 2019 when the Vatican issued a document that firmly rejected the existence of trans identities, claiming gender fluidity posed a threat to traditional family structures.
There was some hope that the Catholic Church would change its approach to LGBT+ people after Pope Francis became leader in 2013 – however, the Vatican has instead recommitted to its anti-LGBT+ policies and teachings.
It’s been 13 years since Thomas Beatie sat down for his first TV interview and told Oprah — and the world — how he could possibly be pregnant, as a man.
Today, the concept of a transgender man giving birth is hardly novel, although research, education and awareness are still severely lacking. But society has come a long way, and so has Beatie. The father of four, now a stockbroker in Phoenix, spoke to TODAY Healthabout how he thinks the trans community benefited from the media attention his pregnancy garnered, and how he and his family are doing today.
“When my story came out, there wasn’t a single person in the public eye as a transgender man — most people had never heard of it,” Beatie, 47, said. “It was a first exposure for a lot of people. And then on top of that, they can give birth! I think exposing the importance of fertility for trans people was a huge eye-opener.”
Thomas Beatie and Nancy Beatie at home May 29, 2008 in Bend, Ore.Kristian Dowling / Getty Images file
In 2008, after he wrote an essay for The Advocate about his pregnancy — a piece he wrote, he said, because he was desperately seeking advice from anyone who had been in his shoes, and fearful that his daughter would be taken away by authorities — Beatie’s story spread around the world. Photos of Beatie cradling his stomach — a bare, enlarged, pregnant stomach — went viral. Requests for TV and magazine interviews rushed in. He wrote a book about his experience titled “Labor of Love,” became the subject of multiple TV specials and even went on to star in a French reality show.
“Everything was a whirlwind,” he said. “But I still don’t regret it.”
After having his first child, Susan, in 2008, Beatie went on to give birth to two more children with his then-wife, Nancy Beatie. The couple separated in 2012, and in 2016 Beatie married his second wife, Amber, who worked at the daycare his children attended. They had a baby together in 2018, to whom Amber gave birth.
Today, Beatie and his family live a relatively quiet life in Phoenix, although Beatie occasionally takes on public-speaking jobs or small acting roles (maybe you saw him as an extra in a U-Haul commercial). His older children — now 11, 12 and 13 — split their time between his house and their mom’s house, about 10 miles away. When they’re all home, they swim together in their pool, play checkers and test out new recipes.
“We’re on this keto kick right now, so we’re trying to make cool dishes together,” Beatie said. “We’re going to make some healthy ice cream.”
Beatie and his ex-wife with their three children at an amusement park in Sweden in 2011. Today the children are 11, 12 and 13.Christopher Hunt / Getty Images file
Yet, more than a decade after his first pregnancy made national headlines, Beatie said he still hasn’t been able to fully shake the “pregnant man” moniker.
“I thought I melted back into society, that I could just walk down the hall and be anonymous,” he said, referring to the halls of his financial office building. But soon enough, word got out about his public past, he said. Not that he minds, exactly.
“I don’t see anything wrong with being a pregnant man,” Beatie said. “I was so proud to be a dad, and I’m still proud to be a dad. I’m so proud that I was the one to bring my kids into the world. It’s kind of like a badge.”
Mostly, he marvels at how much the world, while still very much flawed, has changed since his story was in the spotlight. This was a time before most people understood the concept of gender identity and what it means to be transgender, let alone etiquette for speaking to or about someone who’s part of the trans community. Beatie recalled being misgendered and “deadnamed” by the media and being the butt of talk show jokes. When Beatie sat down for an interview with Barbara Walters, the news icon referred to one of his maternity photos as a “disturbing image.”
“It was really hard when my story came out,” Beatie said. “People were saying things on TV and in the media that if they came close to saying today, they would be immediately fired. I’m just in shock about how wild, Wild West it was back then.”
Despite the challenges of sharing his story and the fame it spawned, Beatie does not regret talking about his pregnancy experience publicly and said he hopes by doing so that he made things a bit easier for the trans men who came after him.
“I wanted to make sure that for my family, and for other people, that this was going to be something that’s doable, that our laws would respect it,” Beatie said. “So I did feel an obligation to continue to fight. I wasn’t about to lay down and say, ‘All right, fine, call me a woman.’”
Yet he acknowledges that even if public perception of his personal experience has shifted, there is still plenty more work to be done to support trans people hoping to start families — more training among health care providers, equitable access to fertility treatments and parental leave, for starters.
“I think a lot of people are still pigeonholed, thinking that if you want to be transgender, you have to completely get rid of all your (reproductive) organs,” Beatie said. “There needs to be discussions about fertility, preservation. Being transgender, you shouldn’t have to lose your right of having a family. You’re entitled to be happy and have a family and be respected.”
Making friends is a lot harder in your adult years than it was in high school and college, and it’s even harder if you’re looking specifically for gay friends. But commenters chimed in with advice after one Reddit user asked for “specific, actionable, constructive advice” for befriending other gays, and many of their tips honed in on the two Gs: groups and Grindr. Read on for their responses, edited for clarity.
“Work and Reddit. … I’ve met one person off Reddit, but he actually knows quite a bit of people, so I’ve been meeting some of his friends little by little.”
“Usually making one friend will lead you to meeting their friends and basically a chain reaction, if you’re lucky. The usual [advice] is [to] join clubs or group activities, even online ones in your area. I used to go to the bars alone, have a drink or two, and basically just talk to strangers. Maybe someone was alone or someone saw me alone. Sometimes I’d run into someone I hadn’t seen in ages and made friends with their friends. It’s best to not go in with high expectations. A couple of times, it was a dud, but I was happy to leave the house.”
“Find your local LGBT center and volunteer and go to events. There are other queer folk looking for friends.”
“Most of the gay friends I have came from Grindr. The only ones that have stayed are the ones that I didn’t hook up with. My roommate got on Facebook, and it suggested to him a lot of the local gays, and he got to know them that way, just by randomly adding them and messaging them on Facebook. He is braver than me in that respect.”
“Reach out to people that you find interesting! My current best friend and I met after he randomly reached out to me on Facebook 3 years ago. Yes, it started out as flirty but turned into a beautiful friendship. Also, join groups. I have a really good friend in Texas I talk to and FaceTime a bunch. We met through the comment section on a post in the Facebook group we were both in. Granted, we are in different states, but I love having her. I also have another gay friend in Texas I met through the same way! Otherwise, hobbies and common interests. Start a new hobby and find people in your community that are also into that hobby. The more you frequent the same place, the higher the chances of running into the same people and becoming friends. Anyway, I need to take my own advice because I need more friends, but I hope this helps.”
“Back when I was a teenager — 32 now — I used to go to gay chatrooms online and talk to gay guys in my local area. Met up with them, and from then on, I’ve met more gay friends. I guess nowadays an online chatroom is equivalent to Reddit, Tinder, Grindr, etc. Or you can go to gay clubs and bars by yourself, if that’s your thing. I know being there by yourself can be a bit weird and intimidating at times, but people would usually try to talk to you, especially if you’re on your own in there.”
“Oddly, Grindr. Just separated ones I was trying to hook up/date [from] other bottoms I just became friends with.”
Sometimes, Noel Arce has trouble remembering his dads.
Not his biological parents — he never met them: His birth mother gave him up as an infant, and he never knew who his birth father was.
But in 1988, he and his brother, Joey, were taken in by Louis Arce and Steven Koceja, a gay couple from Manhattan. Louis was a social worker, and Joey, 2, and Noel, about 10 months old, were in the foster care system.
The boys had been surrendered at New York City’s Metropolitan Hospital. “Our mother and dad were heroin addicts, and they couldn’t really care for us,” Noel said.
During the week, the brothers and Angel, an HIV-positive 3-year-old, lived with Louis and Steven in their Manhattan apartment, and on weekends, they went to the couple’s house in the scenic town of Rosendale, New York, about two hours north.
“It felt very normal, my childhood,” Noel said. “Like the world operated with moms and dads, and two dads and two moms.”
Noel was always free to be himself growing up — to play with Barbie dolls and dress up in frilly costumes. His dads loved to make home movies; in one, Joey and Angel are playing with Tonka trucks and Noel is picking flowers.
“I was very feminine. I’d always participate in girly things, and my dads embraced that in me,” he said. “That really helped me in my development as a child,”
As he got older, Noel realized that was a unique experience.
“I hear people’s stories of coming out and being rejected, being thrown out. That experience for most gay men is a very hard one,” he said. “I’m very blessed to not have had that.”
Louis Arce with his children Joey, Angel and Noel.Courtesy Noel Arce
The time they had together was special, but it was all too brief. Joey and Noel’s adoptions were finalized in 1993. On June 18, 1994, Steven, 32, died of AIDS-related complications. Five days later, Louis, 47, succumbed to the disease.
Noel was just 7 at the time.
Now 33, he says some of the memories of his time with Louis and Steven are fuzzy. He compares them to a train leaving the station, getting smaller and smaller as it pulls away.
Some moments, though, are crystal clear.
“When I look at some of the photos I have, I can remember the day the picture was taken,” he said. “When I see the bedroom, I can remember being there, I remember certain smells — what was cooking that day. And I remember all the Barbies I had.”
One memory in particular stands out: Noel had just turned 6, and, as usual, the family was making a video. “It was like a horror movie, but, you know, silly,” he said. “I dressed up as a witch, and my brother was, like, a devil. And my dad was videoing it, and we were all having so much fun.”
As an adult, he says, he’s better at holding onto the memories. “But I don’t remember the end. I don’t remember them being sick. I don’t remember visiting them in the hospital.”
When Louis and Steven knew their time was running out, they recorded special videos for the boys.
Steven J. Koceja.Courtesy Noel Arce
“There’s a video of them talking to us — explaining how much they loved us,” Noel said. “And there’s videos Louis made for each of us individually. In the video for me, he says, ‘Noel, I know you’re gay.’ And he gives me his thoughts and advice about facing life. I’m so lucky to have that.”
He watched that video for the first time a year after his dads died and, unsurprisingly, didn’t really understand it. About two years ago, he watched it again.
“It was the first time I had an emotional reaction — where I cried,” he said of watching the video.
After Louis and Steven died, Louis’ brother Robert and his wife, Tina, took in the three boys.
When Louis and Steven started to get sick, they had asked Robert and Tina to become the boys’ guardians and started transitioning care.
“Sometimes we’d come over for longer visits,” Tina said. “Other times it would just be the kids and us. We talked to them about what was going to happen, but how do you prepare a child for that?”
She and Louis had known each other since they were kids themselves. “He always, always wanted children,” she said. But, he was an HIV-positive man at a time when treatment options were minimal to nonexistent.
“I said to him, ‘Why would you do this to these kids — taking them in, knowing you have a death sentence, that you’ll disappear on them?” And he said, “Who would know better than me what they’ll face?”
Bringing the boys into the family “changed our whole dynamic forever,” she said. “I was done raising kids by that point, and then there I am, taking these” children in.
But she got much out of the experience, too, she’s quick to add, “maybe even more than the kids.”
“I became involved in AIDS care. I traveled. I met people I never thought I would. I fought for them,” she said. “The man upstairs knew what he was doing bringing us together. It was amazing how my life turned around. If it wasn’t for our family, I don’t know what I’d do.”
Noel, who lives with Robert and Tina in Suffolk County, New York, said he and Joey, who lives nearby, are still very close. Sadly, he doesn’t know what became of Angel, whom he said developed serious emotional problems in adolescence and had to be taken out of the family.
“I don’t know if he’s alive,” he said. “Back then, AIDS was a death sentence. But with the way medication is today, I hope he’s OK — and that he’s happy.”
Noel’s mother was HIV-positive when she was pregnant, and he tested positive for the virus at birth. Eventually, though, he developed his own antibodies and was determined to be HIV-negative.
In April, Noel shared a photo of Joey, Angel, Louis, Steven and himself on the AIDS Memorial Instagram, a page dedicated to sharing stories of those lost to the pandemic.
“We weren’t with Louis and Steven very long before they passed,” he wrote in the accompanying caption. “They never got a chance to see the men we are today but they cared for us very much and gave us a life that we wouldn’t have known otherwise. It’s incredible even now, after all these years, I can still feel what it felt like to be loved that much.”https://iframe.nbcnews.com/VhRU9be?app=1
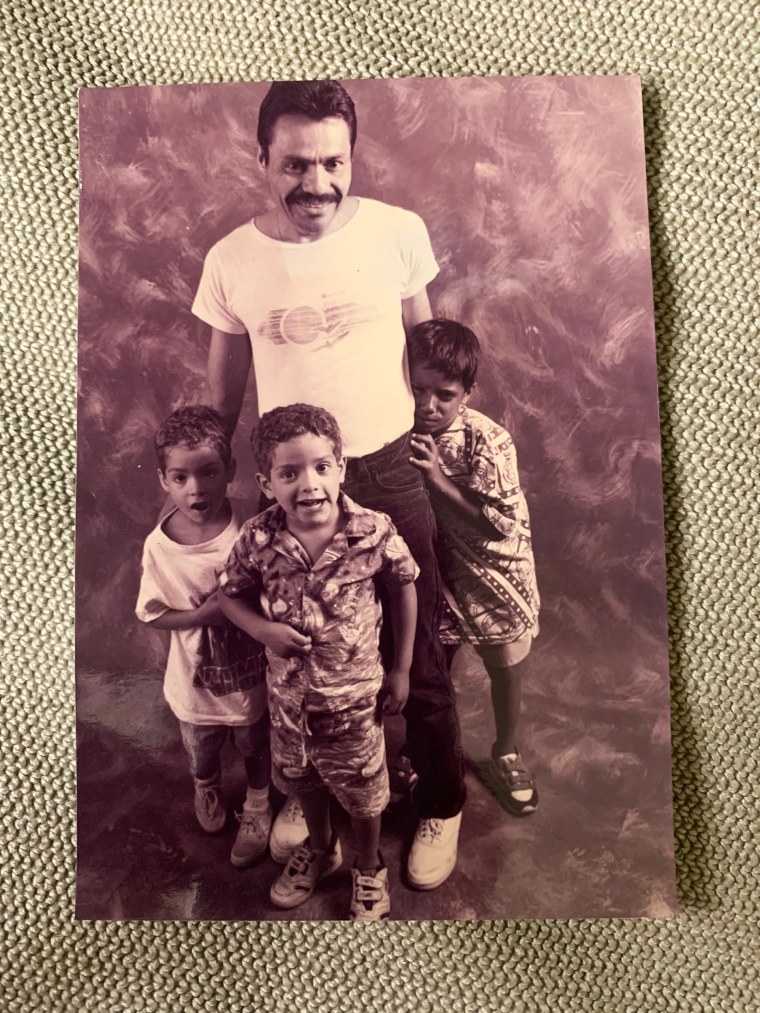
The black and white image included in the Instagram post was from an early ‘90s photo shoot for “Living Proof: Courage in the Face of AIDS”, a collection of portraits published in 1996 by photographer Carolyn Jones of people from all walks of life living with HIV/AIDS.
“I remember the family well,” Jones said of the shoot. “There were not that many families photographed for “Living Proof,” so they are easy to remember. Those three little boys were priceless together. It felt as though they had all somehow miraculously found one another, and there was a lot of love wrapped up in that photo.”
Noel’s post has received hundreds of comments and more than 15,000 likes.
He doesn’t remember how he first came across the AIDS Memorial Instagram account, which NBC News reported on in December for World AIDS Day.
“I think a friend of mine followed that account, and it got recommended to me,” he said. “But when I saw it, I was like, ‘Wow, all these people are telling their stories.’ And I just kind of felt compelled to tell my story, too.”
The response was tremendous, Noel said, adding that it has been particularly meaningful to see comments from people who hadn’t been directly affected by the AIDS devastation of the 1980s and ‘90s.
“I guess I thought that AIDS was a conversation people weren’t having anymore. That no one cared,” he said. “With young people today, they think, ‘Oh, we have medications, we have Truvada, and [HIV] isn’t something to really worry about, right?’ My fear is that it’ll completely be forgotten. But the page keeps it alive. It makes people remember our history and the people who fought for what we have now … And who even died in the process.”
Noel doesn’t know much about how Louis and Steven were able to take in HIV-positive boys in the late ‘80s. “I do know that they fought for us quite a bit,” he said. “I can only imagine how hard it was at that time.”
He has shared other family photos of his dads, his brothers and himself on social media. It’s comforting, he said, but it also churns up immense feelings of loss.
“God really handed me the courage to look at those pictures again,” Noel said. “It had been years — there’s a lot of pain attached to them. But it was a great childhood, it was. I look back now, and I’m like, ‘Wow, I was so lucky.’”
For the past 13 years, Noel has worked in drag, as Violet Storm, playing clubs in Manhattan and out on Long Island. The pandemic put a pause on gigs, but more recently he’s been able to perform again.
Noel Arce during a drag performance as Violet Storm.Courtesy Noel Arce
Knowing his dads were gay, Noel often wonders what they would think of his drag. “Not whether they’d approve of it, because of course they would,” he said. “But, would they think I’m funny? That I’m pretty? Would they like my show?”
He has a lot of questions about his dads that can’t really be answered.
“Like, how did they meet? I want to know the whole love story — I want to hear about those crazy feelings you have when you first meet someone,” he said. “What bars did they go to? Did they have a favorite drag queen? What kind of homophobia did they face back then?”
Tina has been a fount of information about his dads, “but this isn’t really stuff she can tell me.”
He recalled doing a show at the historic Stonewall Inn and wondering if Louis and Steven had gone there back in the ‘80s and ‘90s.
“Every time I do a show, I think, ‘Were my dads here? Did they like this bar? Who did they see perform?’ Sometimes I cry when I think about it,” Noel said. “But they give me a lot of courage, too. Before I go on, I get really, really nervous. And there’s a moment where I have to go on, and I think, ‘I’m just going to back out. I’ll leave. I just can’t do this.’ My heart is racing, I’m so nervous, and then I think of my dads, and I’m like, ‘Just do it. Just let it happen.’”
Noel Arce.Courtesy Noel Arce
While Noel still has a lot of unanswered questions about his dads, he has learned a bit more because of the AIDS Memorial Instagram: Writer and artist Timothy Dean Lee, who follows the page and frequently comments on posts, knew Louis and Steven back in the day.
“When I read Noel’s tribute it was overwhelming,” Lee told NBC News via email. “It gave me answers to what had happened to Louis and Steven — and to the boys. I couldn’t stop crying.”
Lee had met Louis in the 1980s as a graduate student at New York University, where he was studying art therapy and child psychology. He’d often find himself in New York Family Court, where Louis was working as a social worker.
He’d also see Louis at meetings of the AIDS Coalition to Unleash Power, or ACT UP, and protests — and, on occasion, bump into Steven and Louis at the Paradise Garage “dancing the night away.”
“I remember when Louis told me that they were going through the process of adopting the boys,” Lee said. “I knew that adopting for a straight couple was challenging enough, but for a gay couple the challenges were all-consuming. But that certainly didn’t stop Louis and Steven.”
Being a social worker, Lee said, Louis knew the “ins and outs” of the system.
“He was driven. He knew the three boys needed a stable home and love, and he and Steven were more than willing to embrace them as part of their family.”
The last time Lee remembered seeing Louis was about 1990 on the street in the West Village.
“I asked him if he and Steven ever were able to adopt the boys,” he said. “He explained they were still officially foster parents, but they were determined to adopt all three.”
“Louis pulled out his wallet and showed a picture of the kids, saying ‘Yep, Tim, that’s my family.’”
Trafalgar Square’s fourth plinth will welcome an artwork featuring casts of the faces of 850 trans people.
For the artwork, 850 Improntas (850 Imprints), Mexican artist Teresa Margolles will cast the faces of 850 trans people in London and beyond.
The proposed sculpture would highlight people whose “lives are often overlooked”, many of them sex workers, forming one of the world’s highest-profile public art commissions.
The casts will be arranged around the fourth plinth to create a Tzompantli, a skull rack from Mesoamerican civilisations used to display the remains of war captives or sacrifice victims.
Due to London’s weather, Margolles expects the casts to wear away and eventually disintegrate, leaving behind “a kind of anti-monument”, she told the Guardian.
The current artwork featured at Trafalgar Square’s fourth plinth is Heather Phillipson’s The End – a giant replica of whipped cream topped with a cherry, a fly and a drone – which will be on display until September 2022.
Following that will be a sculpture by Samson Kambalu, which is inspired by a 1914 photo of African independence hero and preacher John Chilembwe with English coloniser John Chorley. The sculpture will highlight Chilembwe, making him larger-than-life while Chorley remains life-size, who is wearing a hat in an act of defiance of a colonial rule that forbade Africans from wearing hats in front of white people.
Kambalu and Margolles’ artworks were chosen by the Fourth Plinth Commissioning Group after a public vote of nearly 17,500 people.
Ekow Eshun, the chair of the group, said it received more public votes than ever.