A prominent children’s hospital publicly apologized Thursday for performing cosmetic genital surgeries on intersex infants and pledged to end the practice.
“We recognize the painful history and complex emotions associated with intersex surgery and how, for many years, the medical field has failed these children,” the Ann & Robert H. Lurie Children’s Hospital of Chicago said in a statement. “We empathize with intersex individuals who were harmed by the treatment that they received according to the historic standard of care, and we apologize and are truly sorry.”
The apology, signed by the hospital’s CEO and three head physicians, comes after activists, over a yearslong campaign, called on the institution to ban cosmetic genital surgery on intersex infants, which is irreversible. The signatories also committed to “evolving” their policies going forward and stated that the hospital would not perform such surgeries unless medically necessary or with willful consent from fully informed patients.
“Historically care for individuals with intersex traits included an emphasis on early genital surgery to make genitalia appear more typically male or female,” the statement, published Tuesday, continued. “As the medical field has advanced, and understanding has grown, we now know this approach was harmful and wrong.”
“Intersex” is an umbrella term that refers to individuals born with sex traits or reproductive anatomy that do not fit the conventional categories of male and female. Approximately 1.7 percent of the population fits into this broad category, according to research cited by the intersex advocacy group InterACT.
Intersex activists have long advocated for a ban on medically unnecessary genital surgery for intersex infants. They have argued that the historically common practice — intended to “help” these individuals better fit into society — denies them the legal right to consent to the procedure. According to the Human Rights Watch, 1 in every 2,000 children “is different enough that doctors may recommend surgical intervention to make the body appear more in line” with a conventional male or female.
Along with intersex justice organizations, multiple civil and human rights organizations, like Human Rights Watch and the ACLU, have long condemned these procedures as unnecessary, saying that there is no evidence such practices help individuals better function in society.
Many who were forced to undergo these surgeries report lifelong harm, including higher risks of scarring, loss of sexual sensation and psychological trauma.
While the hospital has not disclosed how many such procedures had been performed over the years, it did state that it had not performed a clitoroplasty on a child or infant in five years.
Intersex activist Pidgeon Pagonis, who was subjected to cosmetic genital surgery at the Lurie Children’s Hospital, was in disbelief after hearing the news.
“Today, what matters is the autonomy of future intersex people and patients,” Pagonis said at a virtual news conference on Thursday. “We couldn’t do the whole country, we couldn’t get Congress to agree with us, but we knew that we could do it at one hospital where it happened to me and so many other people.”
“I’m here to say that we did that, we did that!” Pagonis said.
Pagonis, who identifies as nonbinary and intersex, founded the activist group Intersex Justice Project with fellow intersex activist Sean Saifa Wall. One of the project’s goals was to end these practices across the country, specifically at the Lurie Children’s Hospital, where Pagonis underwent a clitorectomy as a child.
Three years ago, the organization launched a campaign demanding the hospital end this practice, staging multiple protests at its front doors, starting the social media hashtag #EndIntersexSurgery, and organizing phone and emailing campaigns to express members’ concerns.
This watershed moment is only a taste of victory, Wall said Thursday at the news conference.
“We are one step closer to ensuring a world where intersex children can live free from harm,” he said.
Two more Black trans women have been murdered in the US this week, and reports have emerged that a Black trans man was killed in June.
Their deaths mean there have been at least 25 trans people murdered in the US in 2020, just over halfway into the year. The Human Rights Campaign tracked 27 violent fatalities throughout all of 2019.
According to local New York TV station WPIX, 32-year-old Tiffany Harris was stabbed to death in her Bronx apartment early Sunday morning (July 26).
She was initially deadnamed and misgendered by the police and the media, but was correctly identified by people in her community as well as a trans rights group.
NYPD officers responded to a 911 call just after 1.30am and discovered Harris with a stab wound to her chest in the hallway of her building. She was rushed to hospital but was pronounced dead at around 2.20am.
Her death is not being investigated as a hate crime. A man caught on CCTV is wanted for questioning, and is believed to have been in a relationship with Harris.
On Monday (July 27) afternoon, a second Black trans woman was found dead in Baton Rouge, Louisiana.
According to local news outlet The Advocate, Queasha D Hardy was just 24 years old and had been shot in broad daylight. She was found just after 1pm lying in the street with multiple gunshot wounds and passed away at the scene.
Hardy was also misgendered and deadnamed by police and the media after her death, and her next of kin reportedly demanded that she be identified as male despite her living openly as a trans woman.
A Black trans man was murdered last month.
Reports have recently emerged that a Black trans man, Brian Powers, was murdered in Akron, Ohio, on June 13.
According to the Akron Beacon Journal, Powers was killed by a single gunshot and was found on the street outside a church.
Police said they have no leads, but the man’s friends and family believe his death is not being treated seriously because he was Black and transgender.
Powers’s friend Steve Arrington, who works at the Akron AIDS Collaborative, said: “I’m kind of disturbed when they say ‘Black Lives Matter’.
“I say: ‘Whose lives, my life? Or just heterosexual Black people’s lives? What about my LGBTQ brothers and sisters? They’re Black. Do their lives matter?’”
After Harris’ death, Human Rights Campaign said in statement: “There are currently very few explicit federal legal protections for transgender or gender-expansive people.
“Nationally, despite some marginal gains in state and local policies that support and affirm transgender people, recent years have been marked by anti-LGBTQ attacks at all levels of government.
“We must demand better from our community, peers and elected officials and reject harmful anti-transgender legislation appearing at the local, state and federal levels.
“It is clear that fatal violence disproportionately affects transgender women of colour. The intersections of racism, transphobia, sexism, biphobia and homophobia conspire to deprive them of necessities to live and thrive.
“This epidemic of violence that disproportionately targets transgender people of colour — particularly Black trans women — must cease.”
Following the deaths of four trans people – three of whom were Black trans women – in a single week at the start of July, HRC said it has “never seen such a high number at this point in the year” since they began tracking this data in 2013.
Black trans army veteran Jamel Young is suing the New York Police Department for their “dehumanising” treatment of him during what began as a routine traffic stop in 2019.
Young, 33, had driven to New York from Atlanta, with his girlfriend, in March 2019.
His ordeal began when, after dropping his girlfriend at a friend’s apartment, he began looking for somewhere to park.
When an unmarked NYPD car pulled him over, Young said he didn’t panic.
“I’m feeling like, OK, I didn’t do anything wrong, whatever this is I’ll take care of it,” Young toldBuzzFeed News.
But the US citizen said was still aware that as a Black man in the Bronx late at night, he needed to be careful. “The only thing on my mind is to comply,” he said.
It was after he disclosed to the police officers that he is transgender that the problems began.
According to Young’s lawsuit against the corrections department and the NYPD, filed last month, the police then misgendered, assaulted and sexualised him. Officers also dismissed his fears for his safety and failed to provide for his basic needs, Young alleges.
His case comes one year after New York City was sued over the death of Layleen Polanco, the Afro-Latinx trans woman who died in solitary confinement in Rikers Island prison.
After asking him “basic traffic stop questions”, police asked Jamel Young if he had a gun on him. He did – and though it was registered, what Young didn’t know was that he needed a separate license to take it out of Georgia.
He also didn’t know whether the gun was in the car with him or if it was in the bags he’d dropped with his girlfriend at his friend’s house. He says he also didn’t know that you need a different license to carry a gun on your person and in your vehicle.
The police – who arrest hundreds of tourists every year for bringing firearms to New York, which has some of the strictest gun laws in the country – placed him under arrest.
“I didn’t know or think that I was doing anything wrong, I thought I was doing everything completely, 100 per cent right,” Young said.
As police pulled him from his car, he panicked and told them he’s trans – hoping they’d be respectful. But instead, several officers grabbed his chest and crotch like they were “trying to confirm” that he’s trans.
Young also alleges another officer sexually assaulted him while transporting him to the police station.
His lawsuit also alleges that police officers joked about him being trans and called him “he, she, her, him, miss and sir” at various points in the night.
Young was taken to prison, where his problems continued. He said he feared for his life, and that when he asked his legal-aid lawyer what to do, he was told to tell officers that he was female.
“I felt worthless,” he told BuzzFeed News. “I felt like all those triggers that trans people try so hard to manage throughout the transition, all of it just exploded.”
The NYPD said in a statement: “NYPD recognises and supports the rights and dignity of transgender and gender non-conforming persons. We endeavour to treat all individuals with the utmost respect.
“This lawsuit will be reviewed in the normal course when service is effected.”
Jamel Young said he’s suing because he wants to see changes that will ensure the safety of transgender people in custody.
“I’m not asking for anything special. I don’t think I need to get coffee three times a day. I literally just need my safety,” he said.
When Theresa Jean Tanenbaum changed her name last summer, she realised she was now deadnamed in two decades worth of professional accomplishments.
A trans woman who transitioned in her 40s, Tanenbaum is a designer and scholar of human-computer interactions who’s been published in dozens of journals.
Not only was her deadname a traumatic reminder of her past, in her own words, but having new work published in her correct name meant she would lose the continuous record of her life’s work.
“I was faced with what felt like an impossible choice: to abandon past work, or accept that I would never escape an identity that for decades had felt like a prison,” Tanenbaum writes for Nature.
So, she decided on a third path: she would contact her past publishers, a total of 15 legal entities that are responsible for 87 different publications, and ask them to update their records.
But Tanenbaum immediately encountered a problem: none of the 83 academic publications she had published research with would agree to change her name in their digital archives.
A year on, and Tanenbaum explains why this refusal is so dangerous.
“Public connections between my name and my deadname put me in the way of other, more concrete harms,” she wrote for Nature – a journal published by Springer Nature, which was one of those that refused to update her name.
“Fifteen countries criminalise the gender identity or expression of trans people — a crime that in some cases carries the death penalty.
“And until the Supreme Court ruling [making it illegal to fire workers for being gay or trans], at least 20 US states did not protect transgender individuals against employment discrimination. Even when the law protects us, de facto discrimination remains real.”
Though she was initially refused, Tanenbaum has been persistent. The Association of Computing Machinery (ACM) Digital Library, which is the largest scholarly repository of computing, is where most of her work is published.
Digging into their name-change policies, Tanenbaum got in touch – and the ACM board agreed to set up a working group, consisting of her, board members and three other trans scholars, to look into tackling the issue of drafting an inclusive name-change policy.
There were more problems ahead. One of these, Tanenbaum writes, is that cis people object to trans people updating their names because of an “insinuation that the request is a form of deceit or fraud”.
But in fact, Tanenbaum says, it’s the opposite.
After 16 months, the working group have an inclusive name-change policy approved by lawyers and voted through by the rest of the ACM board.
“The plan is for the ACM to update all publicly accessible digital materials related to an author whose name has been changed,” Tanenbaum explains, with the caveat that a previous version remains available in a separate repository, in case of legal challenges regarding the work.
Tanenbaum concludes: “When implemented, it will be, to my knowledge, a first in the publishing world: a trans-inclusive approach to retroactively changing author names on public records.
“These changes will not completely solve the problem of being deadnamed, outed and misgendered. However, it could make the often traumatic, frustrating and dehumanising process of transitioning less fraught.
“That will allow people like me to spend more time doing the scholarship that we’re trained to do, and less time fighting to be called by our names.”
A transgender man is suing the University of Maryland Medical System in federal court, claiming his rights were violated when his gender-affirming surgery was canceled by one of the hospital system’s subsidiaries.
Jesse Hammons was scheduled to have a hysterectomy in January at the University of Maryland St. Joseph Medical Center in Towson. The procedure, routinely performed on cisgender women at the same hospital, was deemed medically necessary for Hammons, who had been diagnosed with gender dysphoria. However, about a week before the scheduled surgery date, the center canceled the procedure because it “conflicted with the hospital’s Catholic religious beliefs,” according to the lawsuit.
Plaintiff Jesse Hammons.Jason Chesnut / ACLU
“Defendants canceled the surgery based on a discriminatory and unconstitutional application of Catholic religious doctrine,” the suit states. “When they canceled Mr. Hammons’ medically necessary surgery, Defendants thus treated Mr. Hammons — as a man who is transgender — differently from nontransgender patients who require medically necessary hysterectomies for other medical conditions.”
The lawsuit, filed Thursday in the U.S. District Court for the District of Maryland, claims that by canceling the surgery, the hospital violated the Constitution’s First and 14th Amendments and the Affordable Care Act’s ban on sex discrimination in health care.
‘Private’ or ‘taxpayer-owned’?
St. Joseph Medical Center, a historically Roman Catholic institution just north of Baltimore, was founded over 100 years ago and was fully acquired in 2012 by the University of Maryland Medical System. UMMS, which maintains that it is a private, nonprofit organization, received over $40 million in “state appropriations” in 2018, according to its most recent annual report, and Maryland’s governor appoints members of the UMMS board.
When UMMS acquired St. Joseph Medical Center, the hospital system vowed to retain the hospital’s “Catholic identity,” which today means it still follows the Ethical and Religious Directives for Catholic Health Care Services, or ERDs, faith-based health guidelines that ban procedures like abortion, euthanasia and gender-confirmation procedures.
Michael Schwartzberg, director of communications for the University of Maryland Medical System, told NBC News in an email that he would not comment on the specifics of pending litigation, but he disputed the claims of the ACLU, which is representing Hammons, that UMMS is “taxpayer-owned.”
“UMMS is a privately-held corporation (since 1984), and SJMC is a privately-held, not-for-profit hospital, and SJMC is mandated to abide by the ERDs,” Schwartzberg said, noting that all Catholic hospitals in the U.S. are bound by the ERDs.
“All physicians and advanced practitioners seeking privileges at UM SJMC agree to abide by the ERDs prior to the granting of privileges,” Schwartzberg said.
Joshua Block, a senior staff attorney with the ACLU LGBT & HIV Project and the lead attorney in Hammons’ case, disputed Schwartzberg’s characterization of UMMS as private, claiming that the medical system is de facto controlled by the state of Maryland. Citing its receipt of taxpayer funds and its largely governor-controlled board, Block argued that the UMMS is bound by the Constitution’s church-state separation.
Hammons’ complaint cites a 1995 Supreme Court ruling that found that Amtrak, being a government-created private corporation, had a responsibility to uphold the First Amendment.
In that ruling, Lebron v. National R.R. Passenger Corp., Justice Antonin Scalia wrote that when the federal government creates a corporation “and retains for itself permanent authority to appoint a majority of the directors of that corporation, the corporation is part of the government for purposes of the First Amendment.”
Block said that Hammons’ lawsuit “raises all the same fact patterns about sex discrimination against transgender patients in the context of transition-related surgery at hospitals, but it also has this added feature where it’s not just a private religious hospital but part of the University of Maryland hospital system.”
“So not only does it violate statutes against discrimination, but the Constitution — both the Equal Protection Clause and the Establishment Clause,” he said.
Block said the ACLU had the case ready soon after Hammons’ surgery was canceled in January but paused because of coronavirus court delays. He said June’s landmark Supreme Court decision in Bostock v. Clayton County, Georgia — which found that federal job discrimination protections extend to LGBTQ people — has only made the filing stronger.
“The landscape after Bostock certainly strengthens our claim under the ACA,” Block said, referring to a ban on health care sex discrimination contained within the Affordable Care Act.
The Trump effect
Even after the Bostock decision, the Trump administration is continuing its effort to reverse Obama-era transgender protections in health care.
Chase Strangio, ACLU’s deputy director for transgender justice, said the legal interpretation advanced through years of Trump administration policies — that sex discrimination bans in various laws do not prohibit discrimination based on sexual orientation and gender identity — won’t go away on its own.
“There’s nothing self-executing about the decision,” Strangio said of the landmark Bostock ruling. “Implementation of civil rights laws is a multi-year project always, because we have strong resistance to them.”
He said he expects that courts will be called upon to enforce the precedent-setting finding central to the Bostock decision: “It is impossible to discriminate against a person for being homosexual or transgender without discriminating against that individual based on sex.“
A coalition of Democratic state attorneys general sued the Trump Administration on Monday, seeking to block next month’s implementation of a rule overturning Obama-era protections for transgender people against sex discrimination in health care.
New York Attorney General Letitia James, leading the group of 23 states, said the change affecting the Affordable Care Act’s anti-discrimination section would give health care providers and insurance companies carte blanche to refuse treatment based on factors such as gender identity.
James also raised concerns that women could be denied access to abortion under the revision, which takes effect Aug. 18, and that non-English speakers will be deprived of information through a change to requirements that insurers print materials in a variety of languages.
“This is just the latest attempt by President Trump and his administration to unlawfully chip away at health care for Americans after failing to repeal the ACA time after time,” James told reporters in a conference call announcing the lawsuit.
The lawsuit, filed in Manhattan federal court against the Department of Health and Human Services, secretary Alex Azar and civil rights chief Roger Severino, seeks an injunction to stop the rule from taking effect. The attorneys general argue it violates the Fifth Amendment’s equal protection clause.
A message seeking comment was left with a spokesperson for the department.
The Trump Administration pushed ahead with the rule change even after a Supreme Court ruling last month barring workplace sex discrimination against LGBT people, moving to show Trump’s religious and socially conservative supporters that he remains committed to their causes ahead of the November election.
Under the change, Health and Human Services said it will enforce sex discrimination protections “according to the plain meaning of the word ‘sex’ as male or female and as determined by biology.” That rewrites an Obama-era regulation that sought a broader understanding shaped by a person’s internal sense of being male, female, neither or a combination.
The lawsuit brought by the attorneys general is part of an expected flurry of lawsuits challenging the lawsuit, including one filed last month by the LGBT civil rights organization Lambda Legal. Such groups say explicit protections are needed for people seeking sex-reassignment treatment, and even for transgender people who need care for common illnesses such as diabetes or heart problems.
California Attorney General Xavier Becerra and Massachusetts Attorney General Maura Healey, both frequent Trump foes, assisted James in crafting the lawsuit. Becerra said implementing the rule while coronavirus continues to rage across the country is especially cruel.
“This is a mean and unconstitutional rule in any context,” Becerra said. “But authorizing discrimination in our health care system at this time, when our nation is suffering through a pandemic, is unbelievably immoral.”
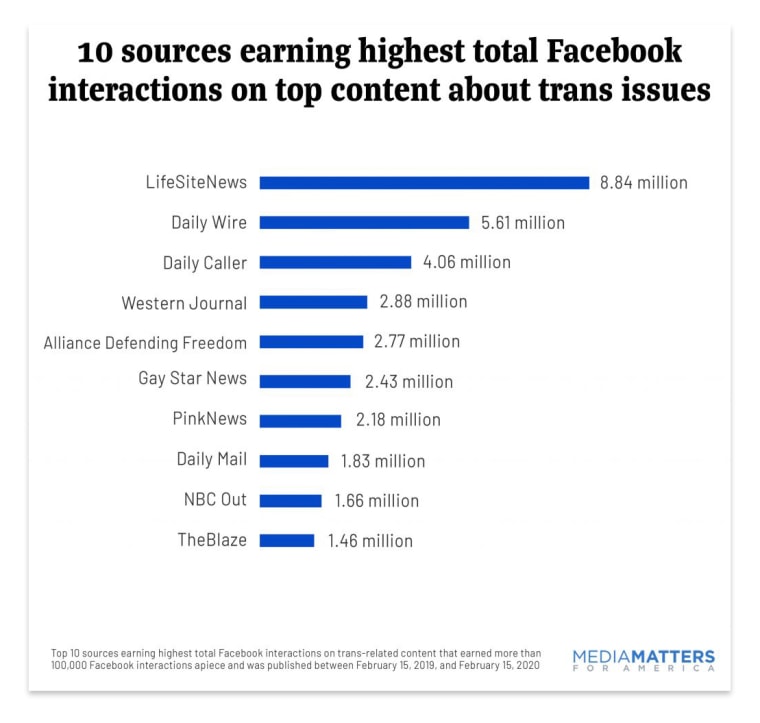
Anti-transgender Facebook content shared by right-wing news sources generated more engagement than content from pro-transgender or neutral sources combined, according to a Media Matters for America study of 225 viral social media posts.
That means the majority of Facebook interactions with those viral posts — over 43 million of 66 million shares, comments and reactions over the span of a year — were on items posted by anti-trans websites like LifeSiteNews, Daily Wire and Daily Caller, according to the report.
The majority of Facebook interactions with content about transgender topics were on items posted by virulently anti-trans websites.Media Matters for America
“Facebook users are getting a totally biased and factually inaccurate understanding of the multitude of issues that impact trans people,” said Brennan Suen, Media Matters’ LGBTQ program director and one of the study’s authors. Suen pointed to an October Pew poll showing that a majority of Americans get news from Facebook.
In total, seven of the top 10 sources for interactions on popular transgender Facebook content were anti-trans sites. Just three LGBTQ-oriented sources appeared in the top 10: PinkNews, Gay Star News and NBC Out.
LifeSiteNews, Daily Wire and Daily Caller dominated these interactions.Media Matters for America
Trans activist and writer Raquel Willis said she was unsurprised by the finding that Facebook interactions about transgender issues are dominated by sources that oppose transgender rights and degrade transgender individuals.
“Narratives that further our demonization, that further confusion, are still the ones that often carry the most weight in our society,” Willis said. “Blood is on the hands of the Mark Zuckerbergs and the people who don’t want to hold these platforms to a humane standard.”
“Actual lives of marginalized people are at stake,” she added.
Suen said anti-transgender content that “lies about best practice medical care for trans youth” could “enable adults to do harm to their own children and deprive trans youth of affirmation and care that can be life saving.”
“Transphobic discourse online contributes to this dangerous rejection of trans children, real world harassment of trans peopleand harmful policies — and it contributes to a social and political culture that continues to demonize and fail the trans community,” Suen added.
Facebook did not respond to NBC News’ request for comment on Media Matters’ findings.
The Media Matters for America study examined 225 articles, blog posts and videos about transgender topics that had 100,000 or more Facebook interactions and were posted from February 2019 to this February. The liberal nonprofit used the social media analytics website BuzzSumo to identify the viral transgender-related content.
Fifty-six percent of these 225 primarily English-language articles, posts and videos were published by right-leaning sources, the report found. Conservative posts comprised the top five most-interacted-with pieces of trans content and 14 of the top 20.
LifeSiteNews, Daily Wire and Daily Caller dominated these interactions. Stories about transgender participation in sports and medical care were particularly high ranking, generating about 37 percent of all interactions, the report found.
Suen said right-wing and anti-trans content flourishes on Facebook, in part, because the network has failed to fully crack down on “coordinated, inauthentic behavior,” which Facebook’s head of cybersecurity policy, Nathaniel Gleicher, defined as “when groups of pages or people work together to mislead others about who they are or what they are doing.”
Last October, Judd Legum, founder of the liberal news site ThinkProgress, reported in Popular Information that 14 large Facebook pages, like Conservative News (which has nearly 500,000 followers), all of which had no apparent link to the Daily Wire, would “exclusively promote content from the Daily Wire in a coordinated fashion.”
Following Legum’s investigation, Facebook pages like Conservative News, which had allegedly promoted Daily Wire’s content in a coordinated fashion, now contain a disclaimer: “Confirmed Page Owner: DAILY WIRE.”
In an op-ed published this month titled “Facebook Does Not Benefit From Hate,” the company’s vice president of global affairs, Nick Clegg, wrote, “When content falls short of being classified as hate speech — or of our other policies aimed at preventing harm or voter suppression — we err on the side of free expression because, ultimately, the best way to counter hurtful, divisive, offensive speech, is more speech.”
“Exposing it to sunlight is better than hiding it in the shadows,” added Clegg, a former deputy prime minister in the U.K.
Sex education may be starting too late to help young gay men, according to new research.
A study from Rutgers University, published in the Journal of Sex Research, highlights a disparity between young gay men and the straight population when it comes to the age at which people first engage in sexual behaviours.
Queer men become sexually active at an earlier age, researchers find.
Based on a sample of 600 young men who have sex with men, researchers found that on average, same-sex sexual encounters first happen at 14.5 years of age – before straight teens are typically sexual active. Queer men have their first experiences of penetrative sex at age 16 on average – one year earlier than their straight peers.
The researchers wrote: “We found that the mean age of same-sex sexual debut was between 14 and 15 years old, with mutual masturbation occurring earliest on average among this sample, followed by oral sex performed and received occurring at approximately age 15.
“Notably, we found that the debut of same-sex anal intercourse was approximately age 16, which is younger than the national mean of 17 for vaginal intercourse among heterosexual men in the United States.”
Queer Black and Hispanic men are also more likely to report an earlier age for the start of sexual activity.
Men who have sex with men are sexually active from an earlier age on average
The study, which includes only “self-identified consensual behaviours,” also found that approximately 19 per cent of young men who have sex with men indicated that their first sexual intercourse before age 13 – more than double the upper range of national estimates.
Caleb LoSchiavo, doctoral student at the Rutgers School of Public Health, said: “As many schools are forced to redesign their classrooms and curricula to accommodate socially distanced or remote learning for COVID-19, this may be the perfect time to consider implementing comprehensive sex education programming to provide age-appropriate sexual health education for people of all genders and sexual orientations.”
The research also concludes that providers working with young gay men of all ages should consider beginning routine testing for HIV and other sexually transmitted diseases at earlier ages than previously indicated, particularly among youth of colour.
Perry N Halkitis, dean of the Rutgers School of Public Health, said: “Our results suggest that health care providers can play an active role in mitigating sexual and health behaviours that are associated with the early onset of same-sex sexual behaviours; to date the medical profession is ill equipped to address the needs of LGBT+ people.”
Ever since Perriviia “Black Butterfly” Brown moved into her Memphis, Tennessee, apartment in 2015, she has been afraid to sit on her front porch. A Black transgender woman who is partially blind, Brown said she doesn’t feel safe in her neighborhood. She said she often deals with transphobic abuse when she ventures to the nearby grocery store.
“I just stay in the house and mind my business,” Brown, 46, told NBC News. “If I have someone come over, they just have to come over on the inside. I would love to entertain on the outside, but it’s … so violent out here, and you don’t know who likes you and who don’t like you, and you don’t know if they got a hatred against trans women.”
Despite her fear, Brown considers herself lucky to have a home. A 2018 Human Rights Campaign report noted that 41 percent of Black transgender respondents reported experiencing homelessness at some point in their lives, a rate five time higher than the general U.S. population.
“If you are experiencing the intersection of racism and transphobia that leads to social and economic marginalization without access to some kind of permanent housing support, it’s going to be very difficult to fight to try and access that stability that a lot of people in our country take for granted.”
DYLAN WAGUESPACK
But thanks to a recent campaign that has raised over $250,000 to build a small neighborhood of 20 “tiny homes” for Black trans women and nonbinary people in the Memphis area, Brown may soon own her own home — one with a porch where she can sit outside unafraid.
“Tiny homes” are a rising trend made popular with reality TV shows like HGTV’s “Tiny House Hunters.” Seen by some as a path to affordable, minimalist living, tiny homes are pre-made studio structures, sometimes converted from sheds, that cost a fraction of the price of a traditional home.
The project is the brainchild of Memphis-based My Sistah’s House, which helps Black transgender women and nonbinary people access safe housing. The small nonprofit also helps individuals with bail assistance and the legal processes around transitioning.
In June, the group launched a GoFundMe page and quickly exceeded its $200,000 goal in a matter of weeks, according to My Sistah’s House cofounder Kayla Gore.
Since its founding in 2017, My Sistah’s House has provided temporary shelter to those in the Memphis area but has struggled to help them access permanent housing, Gore said. Many of the organization’s clients have been turned away from homeless shelters due to their transgender identity, she said, adding that long-term housing projects are necessary to lift the Black trans community out of an endless cycle of homelessness and poverty.
“It’s been super overwhelming to see the support that’s coming in so fast and so rapidly,” Gore said. She hopes the project will serve as a model for other advocacy organizations that want to help trans people own their own homes.
Transgender homeownership
Homeownership is low among transgender people: The 2015 U.S. Transgender Survey, which included interviews with nearly 28,000 trans individuals across the U.S., found 16 percent of transgender respondents reported owning their homes, compared to 63 percent of the general public at the time.
My Sistah’s House is among a handful of trans-led, grassroots groups that are working to create long-term housing solutions for Black trans women and nonbinary people in the South.
Trans United Leading Intersectional Progress, or TULIP, is a nonprofit collective creating housing solutions for trans and gender-nonconforming people in Louisiana.House of Tulip
In Atlanta, a campaign called the Homeless Black Trans Women Fund, organized by trans activist Jesse Pratt López, has so far raised over $2.7 million of its $3 million goal to create secure, long-term housing for Black transgender women. In Louisiana, Trans United Leading Intersectional Progress, or TULIP, is more than halfway to its goal of raising $400,000 to purchase and restore a six-bedroom house (to be named “House of Tulip”) that will provide a pathway to home ownership for trans and gender-nonconforming people in New Orleans.
“Housing really is this first thing that is such a necessity for people to be able to access all of these other things,” according to Dylan Waguespack, co-founder of TULIP and public policy director for True Colors United. “If you are experiencing the intersection of racism and transphobia that leads to social and economic marginalization without access to some kind of permanent housing support, it’s going to be very difficult to fight to try and access that stability that a lot of people in our country take for granted.”
‘There’s so many roadblocks’
The low rate of homeownership and high rate of homelessness for transgender Americans are connected to the disproportionate discrimination, unemployment and incarceration they face, which can all cascade into a cycle of poverty, according to advocates.
Rebeckah Hill, a Memphis-based rapper, is familiar with this cycle of poverty. A Black trans woman who has experienced homelessness on and off since her early 20s, she has been unable to get her name and gender updated on her government ID, find a stable job and secure housing, or even build the credit necessary to qualify for her own home.
“I can’t get into an apartment now,” she said. “I’m 31 years old. I’ve never had my own place to stay.”
Black trans people have an unemployment rate more than three times that of the general population, and half of these individuals reported “feeling forced to participate in underground economy for survival,” according to a 2018 American Psychological Association report. When people turn to the “underground economy,” which includes sex work and drug sales, they then risk going to jail or prison, and a criminal record is often another barrier to obtaining long-term housing. According to the U.S. Transgender Survey, the rate of Black trans women who were incarcerated in the course of a year was 10 times the rate of the general public.
In May, Hill was incarcerated on a pending drug case. After a week in jail, she was bailed out by the Official Black Lives Matter Memphis Chapter and My Sistah’s House, which also helped her find a room in a temporary rental. Having a felony on her record, she said, has made it difficult for her to qualify for public housing and climb out of the cycle of poverty.
“There’s so many roadblocks,” Hill said. “It makes my head hurt.”
A landmark Supreme Court ruling issued last month found that Title VII of the Civil Rights Act of 1964 prohibits workplace discriminationbased on sexual orientation and transgender identity. While the decision was welcome news to LGBTQ advocates, Gore noted that many Black trans women still lack access to quality education and job training that will help them begin a decent-paying career that would in turn allow them to qualify for an apartment or mortgage.
“A big portion of the folks that we serve participate in survival sex or sex work, therefore, they don’t have verifiable income,” Gore said. “So that’s the reason that they can’t get housing or they’re underemployed, in a sense that they don’t necessarily have access to equitable jobs that will provide them an income that is enough to obtain stable housing.”
Currently, federal law does not explicitly prohibit discrimination based on gender identity in private housing, and at least 25 states do not have state-level protections against such discrimination, according to Movement Advancement Project, an LGBTQ think tank. While an Obama-era rule protects transgender people from discrimination in federally funded housing, the Trump administration announced it intends to reverse this measure, which could result in trans women being assigned to men’s homeless shelters.
Trans women who cannot access stable housing often seek shelter in hotel rooms, according to Hill, who said hotel managers often turn them away “because we’re automatically assumed to be sex workers.”
Even when trans people meet the requirements to qualify for an apartment, they frequently report dealing with discrimination from housing providers, advocates say. According to the 2015 National Transgender Discrimination Survey, 19 percent of respondents reported being refused a home or apartment, and 11 percent reported being evicted due to their gender identity or gender expression. A 2017 Urban Institute study that relied on paired testing found that housing providers were less likely to tell transgender people about rentals. The study found that rental seekers in the Washington, D.C., metro area who told housing providers they were trans were less likely, on average, to be informed about available rentals than those who didn’t.
When Brown applied for her Memphis apartment five years ago, she said she presented as a man to avoid any potential discrimination.
“It made me feel nervous, it made me feel like I’m doing something wrong, and it made me feel like I was an outcast,” she said. “I had to play the role that they wanted me to play, the role to just give me a place to stay.”
Recent studies indicate that the lack of access to secure housing and employment often puts Black trans people at a dangerous crossroads where they are vulnerable to violence. Between January 2013 and July 2020, Human Rights Campaign, an LGBTQ advocacy group, has tracked at least 180 cases of trans and gender-nonconforming people being violently killed in the U.S., with trans Black women accounting for approximately 70 percent of the deaths.
The violence Black trans women endure is directly related to housing insecurity, Gore said, adding that the COVID-19 pandemicwill likely exacerbate the situation.
“That’s because we’re trying to maintain our housing, so we’re doing things that may be a little risky in order to survive and make sure that we do have housing,” she said.
Hill knows this violence firsthand. “I’ve been stabbed in my chest. … I have been shot. I have been through a lot,” she said.
At the end of June, Hill became homeless again after her landlord raised her rent. But through My Sistah’s House’s tiny-homes campaign, Hill hopes to soon have a house to call her own.
“I still have an opportunity to do what it is that I want to do,” said Hill, who hopes to build a career as a musician. “Stability right now would be overwhelming for me. I’m crying now, because it feels so good and sounds so good.”
Last year, the House of Representatives passed the Equality Act, a federal bill that would broadly modify existing civil rights legislation to ban discrimination against LGBTQ people in employment, housing, public accommodations, jury service, education, federal programs and credit, but the law has been held up in the Republican-controlled Senate.
In the absence of federal protections that would make it illegal for both private and federally funded housing providers to discriminate on the basis of gender identity, including homeless shelters, there is no universal safety net that protects Black trans people from the cycle of poverty, advocates say.
“We’ll never be able to eliminate discrimination; it will happen,” Waguespack said. “What we do need is recourse for people who experience it; we need access to justice for those folks, and we need federal, state and local dollars to be moving to folks who are actively working to make housing solutions available to communities that experience this kind of discrimination.”
‘We might have our own town’
My Sistah’s House is currently in negotiations to purchase a plot of land in the Memphis area, where the 20 tiny homes will be installed, according to Gore. The next step, she said, is to purchase the homes (at about $10,000 each) and work with a contractor to ensure they meet building codes. The group also plans to raise additional funds to complete the homes’ interiors and furnish them.
“If it’s successful, we might have our own town in a minute,” said Gore, who hopes to have the project complete by the end of 2020.
In the meantime, Brown imagines how her future tiny house will be adorned: pink and white siding with a black butterfly painted on the side, a rose bush and a swing where she can sit on her front porch with friends.
“Having my own key, just turning my own door into my own home,” Brown said of what she looks forward to the most, “and sitting outside on the porch enjoying the fresh air and the butterflies and just smelling fresh air and freshness and freedom that I can own my own home.”