South Carolina became the seventh state last month to permit health care providers to decline to serve people if they feel doing so would violate their religious beliefs.
As a result, more than 1 in 8 LGBTQ people now live in states where doctors, nurses and other health care professionals can legally refuse to treat them, according to the Movement Advancement Project, an LGBTQ think tank. In addition to South Carolina, Mississippi, Alabama, Arkansas, Tennessee, Ohio and Illinois have similar measures in effect.
“The conflict between patient needs and religious directives has been a serious problem in the past, and I don’t see any sign of that issue being resolved quickly and easily.”
JENNY PIZER, LAMBDA LEGAL
Advocates and legal experts say the laws will further raise the barriers to health care for lesbian, gay, bisexual, transgender and queer patients.
“We often are worried that the expansion of religious rights in these contexts will be taken as a license to discriminate,” said Jenny Pizer, the law and policy director for the LGBTQ legal advocacy group Lambda Legal.
Proponents of such legislation, however, say the measures don’t allow providers to discriminate against or target LGBTQ people.
South Carolina state Sen. Larry Grooms, who supported his state’s law, the Medical Ethics and Diversity Act, told NPR in June that “it’s based on procedure, not on patients.”
“This is America, where you should have the freedom to say no to something you don’t believe in,” he told NPR.
Although “religious freedom” or “conscience” measures, as they’re often called, don’t explicitly list LGBTQ people among those who may be refused treatment, advocates say that in practice they are affected disproportionately.
Ivy Hill, the community health program director for the Campaign for Southern Equality, which promotes LGBTQ equality across the South, said transgender people are among those who will be the most negatively affected.
“When we have laws in place that make it easier for providers to discriminate, of course it’s not going to do anything but make it worse,” said Hill, who uses gender-neutral pronouns. “The people who are already on the margins of the margins are going to be the ones who are most deeply impacted by stuff like this.”
Even before the new law went into effect,they said, many trans people they work with in South Carolina struggled to find gender-affirming health care providers in the state willing to help them gain access to hormone therapy, leading some of them to travel to North Carolina to get care.
Hill said doctors usually don’t tell trans people that they won’t treat them for religious reasons, which makes it hard to know how often it happens. Research has found that LGBTQ people, particularly transgender people, are more likely to face medical discrimination.
A study published in 2019 found that 16 percent of LGBTQ adults, or about 1 in 6, reported experiencing discrimination in health care settings. A 2020 survey from the Center for American Progress, a liberal think tank, found that 16 percent of LGBTQ people, including 40 percent of transgender respondents, reported postponing or avoiding preventive screenings because of discrimination.
Maggie Trisler, who works in tech, said she had a great relationship with her primary care provider in Memphis, Tennessee, for about a year and a half in 2016 and 2017. He asked her in-depth questions about her health and the band she plays in, and he said he was going to take his wife to see her play.
Then, in March 2017, Trisler came out to him as transgender, and she said he suddenly became very cold and told her he doesn’t “know anything about the standards of care” for transgender people. He began to blame pain she was having on her weight, she said.
“It suddenly went from the best doctor-patient relationship I’ve ever had to just the absolute least helpful, most frustrating that I’ve had,” she said.
Three months later, Trisler said, the doctor effectively — although not explicitly — told her he couldn’t see her anymore.
“He did say that he was deeply uncomfortable treating me with [hormone replacement therapy], he wasn’t comfortable providing HRT, and if I was seeking that elsewhere, then maybe I should seek medical care elsewhere,” she said.
Trisler added that she was lucky to have good insurance and that it was easy for her to change doctors, although she acknowledged that she is “coming from a rather privileged position” and that what was just a nuisance for her could have been a “critical roadblock” for others.
While LGBTQ people have long faced barriers to health care because of religious refusals, Pizer said, such religious objections can violate both state and federal law in some cases.
Pizer pointed to a 2005 case in which the North Coast Women’s Medical Care Group in Southern California denied infertility treatments to her client Guadalupe “Lupita” Benitez because she is a lesbian. The providers argued that it was within their religious rights to refuse to offer treatment to Benitez, but the California Supreme Court decided that religious rights protected under California law don’t excuse violations of the state’s nondiscrimination law.
The court found that when doctors are “practicing in a particular field and offering services generally, according to patient needs in their field, they can’t pick and choose among patients in ways that violate the nondiscrimination law,” Pizer said.
Pizer said the problem with laws like South Carolina’s Medical Ethics and Diversity Act is that they use broad language that doesn’t give examples of situations in which a religious objection in medicine would violate medical standards or federal law. Many hospitals, including some that are religiously affiliated, receive federal funding. As a result, if they were to provide fertility treatments to heterosexual people and not to LGBTQ people, they would violate Section 1557 of the Affordable Care Act, which the Biden administration hopes to strengthen to better protect access to abortion and gender-affirming services.
Pizer said the issue is becoming more prominent and contentious as Catholic-affiliated institutions control an increasing proportion of the U.S. hospital system. As NBC News reported recently, more than 1 in 7 U.S. hospital patients are cared for in Catholic facilities.
“The conflict between patient needs and religious directives has been a serious problem in the past, and I don’t see any sign of that issue being resolved quickly and easily,” Pizer said. “A hospital that’s operating in a community to serve the community more broadly should not be imposing their religious beliefs on people that are not part of that faith or that are at the hospital for medical services, not religious services.”
In March 2020, when the COVID-19 pandemic was ravaging the world, a poster appeared in several places in Hyderabad, India. The poster warned, “Do not allow Kojjas, Hijras [an Indian transfeminine community] near the shops. If you talk to them or have sex with them, you will be infected with CoronaVirus. Beat & drive them away or call 100 [the emergency police contact in India] immediately. Save people from CoronaVirus Hijras. [sic]”
Several transgender-rights activists took note, and eventually, the police responded by removing the posters and launching a probe to identify the miscreants. But, this was not the first time that marginalized communities – especially queer and trans communities – were wrongly held responsible for the spread of a global pandemic and had violence instigated against them.
Unfortunately, it wasn’t the last time either. With the monkeypox virus (MPXV) having recently been declared a Public Health Emergency of International Concern by the World Health Organization (WHO), queer people are once again being discriminated against and stigmatized. Experts believe this will prevent successful public health interventions from controlling the spread of the disease.
Monkeypox Is Not A “Gay Disease”
MPXV is a viral disease that spreads through close contact. According to the Centers for Disease Control and Prevention (CDC), the infection spreads through:
Direct contact with MPXV rash, scabs, or body fluids from a person with MPXV,
Indirect contact, i.e., by touching objects or surfaces that have been used previously by somebody with MPXV,
Through respiratory droplets and secretions.
Although MPXV is not as infectious as COVID-19, more than 16,000 cases have been recorded worldwide, and the number continues to grow.
A July 21 paper published in the New England Journal of Medicine, which analyzed demographics of MPXV infections from April to June 2022, reported that “98% of the persons with infection were gay or bisexual men.”
Similarly, in a tweet dated July 23, WHO chief Tedros Adhanom Ghebreyesus mentioned that “this…outbreak is concentrated among men who have sex with men, especially those with multiple sexual partners.” Ghebreyesus added, “That means that this outbreak can be stopped with the right strategies in the right groups.”
Does this mean queer men are at a higher risk of MPXV infections? Gagandeep Kang, an acclaimed virologist at the Christian Medical College, Vellore, India, told LGBTQ Nationthat ‘men who have sex with men’ are not the only group affected by the disease. “If MPXV was a ‘gay’ disease,” she added, “children would not be infected – which they have been in previous outbreaks of MPXV and this one.”
Kang pointed out that while the MPXV virus has been detected in the semen of affected individuals, it is “not strictly speaking a sexually transmitted disease. It is more of the respiratory and skin-to-skin contact routes that lead to transmission.”
A report by The Mint suggests that most MPXV cases are reported in queer men because of the “demographic’s positive health-seeking behavior.”
Adding to Kang’s comments, Aqsa Shaikh, an associate professor of community medicine at the Hamdard Institute of Medical Science and Research (HIMSR), New Delhi, India, and a public health researcher, told LGBTQ Nation that the data on which current conclusions about MPXV transmission are based is a “very weak level of evidence in epidemiological studies.”
Further, Shaikh cautioned that it is essential to distinguish between “association and causation.”
“Just because two things occur together does not mean one causes the other,” she said. So, according to Shaikh, even if we were to go by the reports that say queer men are disproportionately affected by MPXV, it does not mean “having gay sex or being a man who has sex with a man increases your risk of transmission of the disease.”
However, none of this has stopped people from wrongly touting MPXV as a disease that disproportionately affects queer men. For instance, Muqtada al-Sadr, an influential Shia cleric in Iraq, took to Twitter on May 23 to suggest that MPXV resulted from same-sex behavior.
He also called MPXV “homosexual-pox” and asked that queer people “repent”, Middle East Eye reported.
Al-Sadr is not the only one guilty. Stand-up comedian Dave Chappelle has also been accused of calling MPXV a “gay disease”.
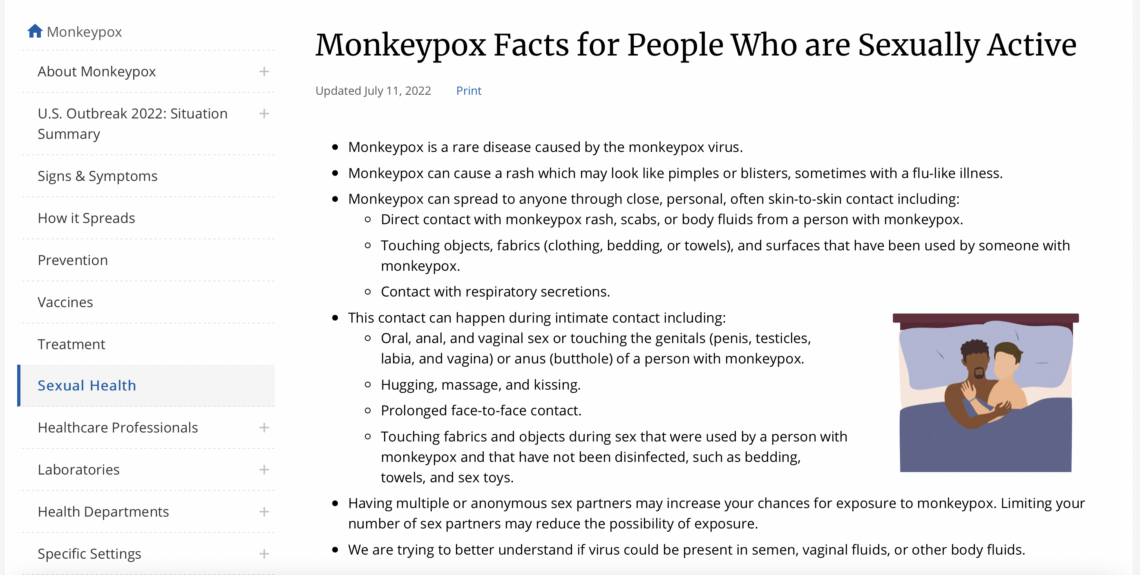
Interestingly, the CDC page on “Monkeypox Facts for People who are Sexually Active” mentions that “[the disease] can spread to anyone through close, personal, often skin-to-skin contact” [emphasis added]. However, the representative picture on the page shows two presumably male bodies in a sexualized position.
A screen grab of the CDC page as of July 25 2022
Remember COVID, AIDS, and SARS
Shaikh alluded that MPXV being portrayed as a ‘gay disease’ is one example of several instances where entire communities have been wrongly shown as carriers of disease and death. As an example, she pointed out how the SARS-COV-2 virus – the causative agent of the COVID-19 pandemic – was colloquially referred to as the ‘Wuhan virus’ in the initial days of the pandemic. This subjected Chinese people to discrimination and xenophobia.
Similarly, Muslims in India were subjected to severe discrimination and islamophobia when a large international gathering of Islamic preachers – the Tablighi Jamaat – in the country’s capital was blamed for a sudden rise in COVID-19 cases across the country. The Printreported, “For days, ‘Tablighi virus’ and ‘Corona Jihad’ trended on Twitter.” A politician from India’s right-wing Hindu-fundamentalist ruling party warned people not to buy vegetables from Muslims.
Perhaps one of the worst instances where queer and transgender persons were stigmatized and discriminated against while losing their lives to deliberate queer- and transphobia was when the HIV/AIDS infection was first identified worldwide.
It has been well-documented how queer and transgender people – along with other marginalized groups like people of color, sex workers, and migrant workers – were portrayed as the key carriers of the virus.
Further, as The New Statesmanhas reported recently, “there was little public will to tackle the virus until people realized that HIV infected everyone, including heterosexuals [sic], equally.”
Shaikh told LGBTQ Nation that this ostracization of marginalized groups negatively affected public-health interventions to control the spread of HIV.
“It doesn’t help because queer and trans people are already stigmatized, and they eventually go further into hiding,” she said, talking about how such stigma discouraged people from getting tested.
Discrimination against queer and trans people resulting from their stigmatization during the early years of the HIV/AIDS pandemic has left marks that are difficult to erase even today.
Science Over Stigma
Shaikh and Kang agree that touting MPXV as a ‘gay disease’ endangers both queer and non-queer people. In the case of queer people, Kang told LGBTQ Nation, “stigmatization leads to lack of or delayed access to care.” On the other hand, she added, “If MPXV is labeled as a ‘gay disease’, then straight people will consider themselves not at risk and be at a higher risk.”
According to Shaikh, tagging MPXV as a ‘gay disease’ is a “distraction.”
“Rather than researching MPXV, we appear to be keener to prove whether it is a ‘gay disease’ or not. A lot of crucial time and resources that could have been utilized in other aspects of epidemiology are getting wasted in this debate,” she said.
A bakery in a Chicago-area suburb that has been the target of vandalism and harassmentdue to a planned family-friendly drag event has now been ordered to stop hosting public events.
“I feel like this is discrimination and a conspiracy to interfere with my business,” Sac said. “Unfortunately, when the attention waned from all the hate this week, they shifted gears and started victim blaming me after we were attacked by a known domestic terrorist who committed hate crimes against us just one week ago.”
Sac says she was first informed that her business was not zoned for entertainment purposes at a Thursday meeting, which she described as “very threatening.” She says city officials also expressed concerns over public resources being used to protect UpRising Bakery after it was the target of a hate crime late last month.
“This issue is about a business conducting activities it was never permitted to conduct,” Village of Lake in the Hills officials said in a statement. “This zoning designation prohibits entertainment in large part due to the close proximity to residential neighborhoods and shared tenant parking.”
“We dispute the letter’s characterization of UpRising programs as ‘entertainment events’ that are prohibited in a B-2 zoning district,” writes senior staff attorney Rebecca K. Glenberg. “Even if that characterization is correct, however, the Village’s sudden determination to enforce the code against UpRising or Ms. Sac based on their exercise of First Amendment rights constitutes unconstitutional retaliation.”
UpRising Bakery became the target of repeated harassment last month after announcing a planned “child-friendly” drag event. “One morning I came in and there was a bag of feces outside,” Sac told Chicago’s ABC7 News. “There was a letter taped to the door that said pedophiles work here.”
The event had to be cancelled after the bakery was vandalized. On July 23, Lake in the Hills Police arrested 24-year-old Joseph I. Collins after he allegedly shattered windows and spray-painted hateful messages on the bakery.
San Francisco has declared a state of emergency, with the city in “desperate need of vaccines” as monkeypox cases skyrocket.
The US has seen around 4,600 confirmed cases of monkeypox across the country. Of these cases, 261 have been detected in San Francisco, representing around 30 per cent of all cases in California.
On Thursday (28 July), San Francisco mayor London Breed said: “We are at a very scary place. And we don’t want to be ignored by the federal government in our need. So many leaders of the LGBT community have also, weeks ago, asked for additional help and support and assistance.”
By declaring a state of emergency, San Francisco will be able to allocate more resources to fight the virus. Breed added that the city was in “desperate need of vaccines”.
San Francisco’s emergency declaration comes as earlier this week World Health Organization (WHO) said the accelerating monkeypox outbreak was a global health emergency, the health agency’s highest level of alert.
Monkeypox has spread around the world in recent months, however the outbreak is concentrated in Europe, and gay and bisexual men are disproportionately affected.
The health department of San Francisco, arguably the LGBTQ+ capital of America, has faced criticism for its response to the monkeypox outbreak because of a lack of public messaging and vaccine information.
The queer community and LGBTQ+ organisations have had to pick up the slack, with the San Francisco AIDS Foundation setting up a monkeypox advice hotline, and creating a vaccine waiting list, rather than forcing those at risk to queue for hours.
But state senator Scott Wiener, who represents the city, said: “San Francisco was at the forefront of the public health responses to HIV and COVID-19, and we will be at the forefront when it comes to monkeypox. We can’t and won’t leave the LGBTQ community out to dry.”
The most visible monkeypox symptom is a red rash with flat marks, with lesions soon rising and filling with puss, before falling off.
According to the NHS, other symptoms include a fever, body aches, chills and swollen glands. Symptoms can take between 5 and 21 days to show and bouts of monkeypox can last for weeks.
The head of the World Health Organization on Wednesday advised men at risk of catching monkeypox to consider reducing their sexual partners “for the moment” following the U.N. health agency declaring the escalating outbreaks in multiple countries to be a global emergency.
WHO Director-General Tedros Adhanom Ghebreyesus said 98% of the monkeypox cases detected since the outbreaks emerged in May have been among gay, bisexual and other men who have sex with men. He called for those at risk to take steps to protect themselves.
“That means making safe choices for yourself and others, for men who have sex with men,” Tedros said. “This includes, for the moment, reducing your number of sexual partners.”
Infectious individuals should isolate and avoid gatherings involving close, physical contact, while people should get contact details for any new sexual partners in case they need to follow up later, the WHO chief said.
The U.S. Centers for Disease Control and Prevention has not suggested that men who have sex with men reduce their sexual partners, only that they avoid skin-to-skin contact with people who have a rash that could be monkeypox.
WHO officials emphasized that monkeypox can infect anyone in close contact with a patient or their contaminated clothing or bedsheets. The U.N. health agency has warned that the disease could be more severe in vulnerable populations like children or pregnant women.
To date, more than 19,000 cases have been reported in more than 75 countries; deaths have only been reported in Africa.
“We know very clearly that one of the main modes of exposure for this particular illness is through direct contact, close contact, skin to skin contact, possibly even face to face contact, exposure to droplets or virus that may be in the mouth,” Dr. Rosamund Lewis, WHO’s technical lead for monkeypox, said.
Andy Seale, a WHO adviser on HIV, hepatitis and sexually transmitted infections, said experts have determined the current monkeypox outbreak is “clearly transmitted during sex,” but he said they have not yet concluded whether it’s a sexually transmitted infection.
Dr. Hugh Adler, who treats monkeypox patients in the U.K., said monkeypox was being transmitted during sex and that sexual networks and anonymous sex with untraceable partners were facilitating its spread.
“It’s just as likely that monkeypox was always capable of transmitting and presenting like this, but it hadn’t been formally reported or so widespread before,” he said.
Last week, British authorities issued new guidance advising doctors that people with just one or two lesions might be infectious with monkeypox, potentially complicating efforts to stop transmission.
The European Union’s health commissioner urged the bloc’s 27 member nations Wednesday to step up their efforts to tackle outbreaks in the EU, which she called “the epicenter of detected cases.”
In a letter to European health ministers obtained by The Associated Press, EU Health Commissioner Stella Kyriakides called for a “reinforced, concerted and coordinated action.”
“There is no time for complacency and we need to continue working together to control the outbreak,” she wrote.
The tasteless, anti-LGBTQI+ comic Dave Chappelle performed five shows at Luther Burbank Center for the Arts in Santa Rosa. It is difficult to believe the LBC staff and board were unaware of Chappelle’s numerous anti-LGBTQI+ comments that are well-documented and for which he has offered no apologies. Chappelle identifies as a so-called “TERF (Trans Exclusionary Radical Feminist)” joining author J. K Rawlings in such dangerous hate speech. These people refuse to accept that we are in the position to declare our gender or lack thereof.
Netflix came under fire for producing and airing two Chappelle shows that feature anti-Trans comments. LGBTQI+ Netflix employees protested – some even quit. Days before the LBC shows comenced, a Minneapolis Chappelle show switched locations as a direct result of a protest organized after Chappelle referred to Monkeypox as “a gay disease.” Chappelle mocked the members of the local LGBTQI+ Community who brought about the move. The original venue apologized to the local LGBTQI+ Community for once welcoming Chappelle and his hate. Chappelle has never backed down, apologized or even reached out to better understand the concerns of he LGBTQI+ Community. Instead, he continues to mock our Community.
The Press Democrat revealed that mere weeks before the five July shows, Live Nation approached LBC with an offer LBC appears to have found unable to refuse. The LBC staff and board claim there was considerable conversation – considerable, but certainly brief and misguided. Did they notice how few dates Live Nation had booked for Chappelle? None in San Francisco or Oakland or Los Angeles. LBC thought they could sneak this past our Community. No doubt comedy venues in big cities find Chappalle as toxic as the LBC staff and board should have.
Luther Burbank Center for the Arts found it necessary to confiscate all audience cell phones before the Chappelle shows. I have attended too many LBC concerts to count but have never had my cell phone taken away before a show. They must have done this so no footage of his anti-LGBTQI+ vitriol would find its way onto social media identifying LBC as the location. Sorry, LBC, you are now forever linked to anti-LGBTQI+ comments.
Should the North Bay’s LGBTQI+ Community allow hate speech and inflammatory comments to be staged in our backyard? Make no mistake – this is not an attack on free speech or about censorship. This is about making LBC aware that Trans people are harmed and even killed as a result of such despicable comments. 2021 saw a record number of Trans-folks murdered. So far this year 57 have been murdered in the United States alone. We once valued this venue, but it’s decision to allow Chapelle a forum for his hate is unacceptable. The LGBTQI+ Community finds Dave Chappelle comments offensive, inflammatory and even deadly.
Let’s stand up to Hate Speech and inform those in power at Luther Burbank Center for the Arts we will boycott the venue. Some shy away from boycotts. If you are amongst them, at least express your opinion by contacting the people listed below.
Let the Staff and Board of Luther Burbank Center for the Arts, its sponsors, those who share the Center’s campus, and elected officials know that such Hate results in harm to members of the LGBTQI+ Community. Email and call, as many as possible and as often as possible.
Call to Action: BOYCOTT Luther Burbank Center for the Arts for Bringing Anti-LGBTQI+ Hate to Sonoma County
The tasteless, anti-LGBTQI+ comic Dave Chappelle performed no less than five shows at Luther Burbank Center for the Arts in Santa Rosa. It is difficult to believe the LBC staff and board are unaware of Chappelle’s numerous anti-Trans comments that are well-documented and for which he has offered no apologies. Chappelle identifies as a so-called “TERF (Trans Exclusionary Radical Feminist)” joining author J. K Rawlings in such dangerous hate speech. These people refuse to accept that we are in the position to declare our gender or lack thereof.
Netflix came under fire for producing and airing two recent Chappelle shows that feature anti-Trans comments. LGBTQI+ Netflix employees protested – some even quit. Recently, a Minneapolis Chappelle show switched locations as a direct result of a protest organized after Chappelle referred to Monkeypox as “a gay disease.” Chappelle mocked the members of the local LGBTQI+ Community who brought about the move. The original venue apologized to the local LGBTQWI+ Community for once welcoming Chappelle and his hate. Chappelle has never backed down, apologized or even reached out. Instead, he continues to mock our Community.
The Press Democrat revealed that mere weeks before the five shows, Live Nation approached LBC with an offer they seen unable to refuse. The LBC staff and board claim there was considerable conversation – considerable, but perhaps, but certainly misguiged. Did they notice how few dates Live Nation had booked for Chappelle. None in San Francisco or Oakland or Los Angeles. LBC thought they could sneak this past our Community. No doubt comedy venues in big cities find Chappalle as toxic as the LBC staff should have.
Imagine, Luther Burbank Center for the Arts confiscated cell phones at the Chappelle shows. I have attended too many LBC concerts to count but have never had my cell phone taken away before a show. They must have done this so no footage of his anti-LGBTQI+ vitriol would find its way onto social media identifying LBC as the location. Sorry, LBC, you are now forever linked to anti-LGBTQI+ comments. Did you think this community could be so easily duped?
Should the North Bay’s LGBTQI+ Community allow hate speech and inflammatory comments to be staged in our backyard? Make no mistake – this is not an attack on free speech or about censorship. This is about making LBC aware that Trans people are harmed and even killed as a result of such despicable comments. 2021 saw a record number of Trans-folks murdered. So far this year 57 have been murdered in the United States alone. We once valued this venue, but it’s decision to allow Chapelle a forum for his hate is unacceptable. The LGBTQI+ Community finds Dave Chappelle comments offensive, inflammatory and even deadly.
Let’s stand up to Hate Speech and inform those in power at Luther Burbank Center for the Arts we will boycott the venue. Some shy away from boycotts. If you are amongst them, at least express your opinion by contacting the people listed below.
Let the Staff and Board of Luther Burbank Center for the Arts, its sponsors, those who share the Center’s campus, and elected officials know that such Hate results in harm to members of the LGBTQI+ Community. Email and call, as many as possible and as often as possible.
Two new cases presented Wednesday at the International AIDS Conference in Montreal have advanced the field of HIV cure science, demonstrating yet again that ridding the body of all copies of viable virus is indeed possible, and that prompting lasting viral remission also might be attainable.
In one case, scientists reported that a 66-year-old American man with HIV has possibly been cured of the virus through a stem cell transplant to treat blood cancer. The approach — which has demonstrated success or apparent success in four other cases — uses stem cells from a donor with a specific rare genetic abnormality that gives rise to immune cells naturally resistant to the virus.
In another case, Spanish researchers determined that a woman who received an immune-boosting regimen in 2006 is in a state of what they characterize as viral remission, meaning she still harbors viable HIV but her immune system has controlled the virus’s replication for over 15 years.
Experts stress, however, that it is not ethical to attempt to cure HIV through a stem cell transplant — a highly toxic and potentially fatal treatment — in anyone who is not already facing a potentially fatal blood cancer or other health condition that would make them a candidate for such a treatment.
“While a transplant is not an option for most people with HIV, these cases are still interesting, still inspiring and illuminate the search for a cure,” Dr. Sharon Lewin, an infectious disease specialist at the Peter Doherty Institute for Infection and Immunity at the University of Melbourne, told reporters on a call last week ahead of the conference.
There are also no guarantees of success through the stem cell transplant method. Researchers have failed to cure HIV using this approach in a slew of other people with the virus.
Nor is it clear that the immune-enhancing approach used in the Spanish patient will work in additional people with HIV. The scientists involved in that case told NBC News that much more research is needed to understand why the therapy appears to have worked so well in the woman — it failed in all participants in the clinical trial but her — and how to identify others in whom it might have a similar impact. They are trying to determine, for example, if specific facets of her genetics might favor a viral remission from the treatment and whether they could identify such a genetic profile in other people.
The ultimate goal of the HIV cure research field is to develop safe, effective, tolerable and, importantly, scalable therapies that could be made available to wide swaths of the global HIV population of some 38 million people. Experts in the field tend to think in terms of decades rather than years when hoping to achieve such a goal against a foe as complex as this virus.
The new cure case
Diagnosed with HIV in 1988, the man who received the stem cell transplant is both the oldest person to date — 63 years old at the time of the treatment — and the one living with HIV for the longest to achieve an apparent success from a stem cell transplant cure treatment.
The white male — dubbed the “City of Hope patient” after the Los Angeles cancer center where he received his transplant 3½ years ago — has been off of antiretroviral treatment for HIV for 17 months.
“We monitored him very closely, and to date we cannot find any evidence of HIV replicating in his system,” said Dr. Jana Dickter, an associate clinical professor in the Division of Infectious Diseases at City of Hope. Dickter is on the patient’s treatment team and presented his case at this week’s conference.
This means the man has experienced no viral rebound. And even through ultra-sensitive tests, including biopsies of the man’s intestines, researchers couldn’t find any signs of viable virus.
The man was at one time diagnosed with AIDS, meaning his immune system was critically suppressed. After taking some of the early antiretroviral therapies, such as AZT, that were once prescribed as individual agents and failed to treat HIV effectively, the man started a highly effective combination antiretroviral treatment in the 1990s.
In 2018, the man was diagnosed with acute myeloid leukemia, or AML. Even when HIV is well treated, people with the virus are still at greater risk of a host of cancers that are associated with aging, including AML and other blood cancers. Thanks to effective HIV treatment, the population of people living with the virus in the U.S. is steadily aging;themajority of people diagnosed with HIV is now older than 50.
He was treated with chemotherapy to send his leukemia into remission prior to his transplant. Because of his older age, he received a reduced intensity chemotherapy to prepare him for his stem cell transplant — a modified therapy that older people with blood cancers are better able to tolerate and that reduces the potential for transplant-related complications.
Next, the man received the stem cell transplant from the donor with an HIV-resistant genetic abnormality. This abnormality is seen largely among people with northern European ancestry, occurring at a rate of about 1% among those native to the region.
According to Dr. Joseph Alvarnas, a City of Hope hematologist and a co-author of the report, the new immune system from the donor gradually overtook the old one — a typical phenomenon.
Some two years after the stem cell transplant, the man and his physicians decided to interrupt his antiretroviral treatment. He has remained apparently viable-virus free ever since. Nevertheless, the study authors intend to monitor him for longer and to conduct further tests before they are ready to declare that he is definitely cured.
The viral remission case
A second report presented at the Montreal conference detailed the case of a 59-year-old woman in Spain who is considered to be in a state of viral remission.
The woman was enrolled in a clinical trial in Barcelona in 2006 of people receiving standard antiretroviral treatment. She was randomized to also receive 11 months of four therapies meant to prime the immune system to better fight the virus, according to Núria Climent, a biologist at the University of Barcelona Hospital Clinic, who presented the findings.
Then Climent and the research team decided to take the woman off her antiretrovirals, per the study’s planned protocol. She has now maintained a fully suppressed viral load for over 15 years. Unlike the handful of people either cured or possibly cured by stem cell transplants, however, she still harbors virus that is capable of producing viable new copies of itself.
Her body has actually controlled the virus more efficiently with the passing years, according to Dr. Juan Ambrosioni, an HIV physician in the Barcelona clinic.
Ambrosioni, Climent and their collaborators said they waited so long to present this woman’s case because it wasn’t until more recently that technological advances have allowed them to peer deeply into her immune system and determine how it is controlling HIV on its own.
“It’s great to have such a gaze,” Ambrosioni said, noting that “the point is to understand what is going on and to see if this can be replicated in other people.”
In particular, it appears that what are known as her memory-like NK cells and CD8 gamma-delta T cells are leading this effective immunological army.
The research team noted that they do not believe that the woman would have controlled HIV on her own without the immune-boosting treatment, because the mechanisms by which her immune cells appear to control HIV are different from those seen in “elite controllers,” the approximately 1 in 200 people with HIV whose immune systems can greatly suppress the virus without treatment.
Lewin, of Australia’s Peter Doherty Institute, told reporters last week that it is still difficult to judge whether the immune-boosting treatment the woman received actually caused her state of remission. Much more research is needed to answer that question and to determine if others might also benefit from the therapy she received, she said.
Four decades of HIV, a handful of cures
Over four decades, just five people have been cured or possibly cured of HIV.
The virus remains so vexingly difficult to cure because shortly after entering the body it infects types of long-lived immune cells that enter a resting, or latent, state. Because antiretroviral treatment only attacks HIV when infected cells are actively churning out new viral copies, these resting cells, which are known collectively as the viral reservoir and can stay latent for years, remain under the radar of standard treatment. These cells can return to an active state at any time. So if antiretrovirals are interrupted, they can quickly repopulate the body with virus.
The first person cured of HIV was the American Timothy Ray Brown, who, like the City of Hope patient, was diagnosed with AML. His case was announced in 2008 and then published in 2009. Two subsequent cases were announced at a conference in 2019, known as the Düsseldorf and London patients, who had AML and Hodgkin lymphoma, respectively. The London patient, Adam Castillejo, went public in 2020.
Compared with the City of Hope patient, Brown nearly died after the two rounds of full-dose chemotherapy and the full-body radiation he received. Both he and Castillejo had a devastating inflammatory reaction to their treatment called graft-versus-host disease.
Dr. Björn Jensen, of Düsseldorf University Hospital, the author of the German case study — one typically overlooked by HIV cure researchers and in media reports about cure science — said that with 44 months passed since his patient has been viral rebound-free and off of antiretrovirals, the man is “almost definitely” cured.
“We are very confident there will be no rebound of HIV in the future,” said Jensen, who noted that he is in the process of getting the case study published in a peer-reviewed journal.
For the first time, University of Cambridge’s Ravindra Gupta, the author of the London case study stated, in an email to NBC News, that with nearly five years passed since Castillejo has been off of HIV treatment with no viral rebound, he is “definitely” cured.
In February, a research team announced the first case of a woman and the first in a person of mixed race possibly being cured of the virus through a stem cell transplant. The case of this woman, who had leukemia and is known as the New York patient, represented a substantial advance in the HIV cure field because she was treated with a cutting-edge technique that uses an additional transplant of umbilical cord blood prior to providing the transplant of adult stem cells.
The combination of the two transplants, the study authors told NBC News in February, helps compensate for both the adult and infant donors being less of a close genetic match with the recipient. What’s more, the infant donor pool is much easier than the adult pool to scan for the key HIV-resistance genetic abnormality. These factors, the authors of the woman’s case study said, likely expand the potential number of people with HIV who would qualify for this treatment to about 50 per year
Asked about the New York patient’s health status, Dr. Koen van Besien, of the stem cell transplant program at Weill Cornell Medicine and New York-Presbyterian in New York City, said, “She continues to do well without detectable HIV.”
Over the past two years, investigators have announced the cases oftwo women who are elite controllers of HIV and who have vanquished the virus entirely through natural immunity. They are considered likely cured.
Scientists have also reported several cases over the past decade of people who began antiretroviral treatment very soon after contracting HIV and after later discontinuing the medications have remained in a state of viral remission for years without experiencing viral rebound.
Speaking of the reaction of the City of Hope patient, who prefers to remain anonymous, to his new HIV status, Dickter said: “He’s thrilled. He’s really excited to be in that situation where he doesn’t have to take these medications. This has just been life-changing.”
The man has lived through several dramatically different eras of the HIV epidemic, she noted.
“In the early days of HIV, he saw many of his friends and loved ones get sick and ultimately die from the disease,” Dickter said. “He also experienced so much stigma at that time.”
As for her own feelings about the case, Dickter said, “As an infectious disease doctor, I’d always hoped to be able to tell my HIV patients that there’s no evidence of virus remaining in their system.”
On Saturday, July 23, World Health Organization Director General Tedros Adhanom Ghebreyesus declared the spread of monkeypox to be a public health emergency of international concern (PHEIC), the organization’s loudest alarm bell signifying an emerging outbreak.
Since early May, more than 15,000 cases of monkeypox have been identified across more than 60 countries. Disease caused by the monkeypox virus typically involves a few days of fever and lymph node swelling followed by a rash, which can leave scars. Most cases in the current outbreak have resolved without hospitalization or the need for medication. As of July 7, there have been three deaths, all of them in Africa.
When the WHO first convened a committee in late June to determine whether monkeypox was a PHEIC. As cases have continued to rise worldwide, the committee reconvened on July 21 — and this time, the outcome was different.
“We have an outbreak that has spread around the world rapidly through new modes of transmission, about which we understand too little and which meets the criteria in international health regulations,” Tedros said when announcing the emergency.
Tedros made the declaration despite the the WHO’s emergency committee for monkeypox, which did not come to an unanimous consensus on whether to declare an emergency. “There are uncertainties on all sides,” said Michael Ryan, executive director of the WHO’s health emergencies program, explaining Tedros’s reasoning in deciding to declare a PHEIC. “He sees a window of opportunity to to bring this disease under control,” said Ryan. The committee offers a recommendation, but ultimately it was Tedros’s decision.
The last time the WHO declared an international emergency was in early 2020, for Covid-19. While the disease caused by the currently spreading monkeypox virus is much less severe than Covid-19 and spreads far less easily, there are good reasons for the WHO to declare an emergency.
For starters, said Ana B. Amaya, an expert in global health governance at Pace University in New York, this monkeypox outbreak is just very different from past outbreaks of the disease. The vast majority of the latest cases have been identified among gay and bisexual men, and sexual contact with multiple sexual partners has emerged as an important risk factor. Scientists are now trying to determine if the virus spreads through sexual fluids like semen and vaginal fluid in addition to the ways it’s already known to spread: via skin-to-skin contact and, to a lesser degree, by respiratory transmission.
Prior to the current outbreak, monkeypox often spread throughout households via close contact and, possibly, shared items like utensils and linens. In the past few weeks, isolatedreports of infections in children, who are thought to be at higher risk for severe outcomes of monkeypox infection, reinforce the worry that without containment, outbreaks often spread beyond the populations where they start.
The prospect that the virus might be spreading in ways not seen before raises the concern that it will surprise us in other ways — for example, by causing severe disease if it reaches certain populations it has not yet reached, like large groups of immunocompromised people, said Amaya. “All of that is really alarming. And that’s why it’s very important for us to have a coordinated response that starts from the WHO level,” she said in a late-June interview, before the WHO’s first meeting to discuss issuing an emergency declaration.
But beyond that, this kind of declaration encourages countries to coordinate to stop the virus’s spread in a few different ways. Here’s how that works.
A public health emergency is not the same thing as a pandemic
To be resoundingly clear: The WHO did not declare monkeypox to be a new pandemic. There’s a difference between a pandemic and a PHEIC.
A pandemic is squishily defined as “an epidemic occurring over a very wide area, crossing international boundaries, and usually affecting a large number of people,” according to A Dictionary of Epidemiology. Public health experts use the phrase “pandemic” to emphasize the global reach of an outbreak. They seem to agree that calling something a pandemic means it demands a coordinated international response — and potentially, that it’s too big to contain.
On the other hand, a PHEIC is a more carefully defined term. It describes a situation that has not necessarily grown out of control, but has the potential to do so.
According to the WHO’s International Health Regulations, an outbreak qualifies as a PHEIC if 1) it’s unusual or unexpected, 2) has potential for international spread, and 3) requires an immediate international response.
The WHO has only declared six PHEICs to date, including Ebola, Zika, and Covid-19.
The monkeypox outbreak easily meets the first two criteria for an emergency: the virus’s spread outside West and Central Africa and among sexual networks are both unusual patterns, and the virus has already spread internationally, with cases now present in about 60 countries. And given that spread, containing monkeypox will clearly require an international response.
Why did the WHO wait to declare an emergency?
Some experts think this outbreak easily met the PHEIC criteria when the WHO first addressed the question about a month ago. Why didn’t it declare an emergency then?
Nearly 50 percent of transgender people travel outside of their state of residence to get gender-affirming genital surgeries, according to a new study from Oregon Health and Science University (OHSU). The percentage could increase as more states put bans against gender-affirming healthcare for trans people in place, the study’s authors say.
The study, published Wednesday in JAMA Surgery, looked at 771 transgender patients who had a vaginoplasty or phalloplasty between 2007 and 2019. It found that 49 percent left their state of residence to get the procedure. People who lived in southern states were more likely to have to leave their home states in order to receive the surgery.
That’s because there’s a lack of surgeons who provide such care in the South. A 2020 studyfound that just 11 doctors in the South could provide such surgeries, and four of the doctors resided in Florida.
The number of such doctors could decrease as more Southern states ban gender-affirming care for trans youth. Genital surgeries aren’t typically performed on young trans people, but some doctors could choose to locate their practices outside of states with such bans in place because the bans increase doctors’ legal and financial liabilities if they treat young patients.
Of additional concern, the OHSU study found trans people who left their states to get surgery ended up paying up to 50 percent more in out-of-pocket medical expenses than those who were able to obtain surgeries in their home states. This included costs for post-surgical visits and foll0w-up care.
Only one of the 771 patients included in the study had their surgery paid for by their commercial health insurance provider, The Hill noted. This suggests that the life-saving surgical procedures may not be affordable for many trans people. Trans people living in transphobic states will face even greater financial and time costs just to receive gender-affirming care.
“We already knew that traveling for health care requires patients to take time off work and pay for travel and lodging on their own, and that it can make receiving follow-up care from qualified providers who are familiar with each patient’s unique needs challenging,” Jae Downing, the study’s lead author, said in a press release.
“This study helps quantify how severely we need more gender-affirming surgeons,” Geolani Dy, an assistant professor of urology and plastic and reconstructive surgery at OHSU School of Medicine, added.
On a sultry Tuesday evening in New York City, Luke Brown excitedly opened a newly delivered bottle of black-and-orange pills, popped his first dose in his mouth, and washed it down with root beer.
Having contracted monkeypox this month, the lanky, bespectacled 29-year-old project manager had been suffering from what he called “the most severe pain of my life” for over a week before he finally was able to obtain a course of antivirals — a treatment he hoped would soon clear up his lesions and alleviate his suffering.
For Brown, this was cause for celebration. But it was also a sobering moment for him to reflect on how, to gain access to this medication, he had to leverage high degrees of personal privilege, medical literacy and self-advocacy that he said he was guiltily aware most people at risk for monkeypox probably lack. Because to join the fortunate few who have obtained this prized medication, called TPOXX, he had to navigate what he characterized as the exasperatingly byzantine maze of the medical and public health system.
“Here we are in the epicenter of an outbreak primarily affecting gay men in the city,” Brown said of his hometown, New York, which as of Thursday had 778 confirmed monkeypox cases out of 2,593 nationwide. “The city that of anywhere in the world should have the most impressive and robust infrastructure to respond to the health care needs of gay men. And at every level it has fallen flat on its face.”
Luke Brown points to a monkeypox lesion on the knuckle of his thumb.Benjamin Ryan for NBC NewsAnother lesion is visible just above Brown’s right eyebrow.Benjamin Ryan for NBC News
Like many of his fellow gay and bisexual men — a demographic that comprises the vast majority monkeypox cases in the global outbreakthat has ballooned to 15,848 cases — Brown said he has grown increasingly appalled and infuriated by the nation’s response to a virus spreading so swiftly that many epidemiologists now believewill likely become endemic in the U.S. and around the world.
Supply of the antiviral is not the problem; there are 1.7 million courses in the nation’s Strategic National Stockpile, according to Dennis Hruby, chief scientific officer of the U.S. pharmaceutical company SIGA, TPOXX’s manufacturer. But the drug, also known as tecovirimat, is not approved by the Food and Drug Administration to treat monkeypox as it is by regulators in the United Kingdom and the European Union; the drug is approved only for smallpox in the U.S.
This is bad news for the Americans with monkeypox who like Brown suffer from excruciating physical pain or other severe outcomes from the infection and who are desperate for treatment to speed their healing. They, and the health care providers who care for them, are up against the U.S. regulatory system.
Even as the Centers for Disease Control and Prevention continues to reduce the red tape that impedes TPOXX access, announcing new changes Friday, public health experts pointed to a complementary means of leveraging the drug’s potential power to alleviate suffering: large clinical trials of the antiviral as a monkeypox treatment.
Plans for such trials are already in advanced stages in Canada, the U.K. and the European Union, according to Hruby. The National Institutes of Health is also planning one in the Democratic Republic of the Congo. But the federal agency’s efforts to launch such research in the U.S. are only in the earliest planning stages.
“This points to a persistent issue we saw during Covid,” said James Krellenstein, a public-health activist and cofounder of the activist group PrEP4All, “where the United Kingdom and European researchers were really able to mount much quicker clinical studies than the United States was.”
Excessive barriers to prescribing
In addition to Brown, NBC News spoke with a dozen people who have taken TPOXX, all of whom suffered from extreme pain before starting the antiviral. They generally reported that within a few days of treatment, their monkeypox symptoms — the pain in particular — began to ease, much to their relief. Most reported no bothersome side effects, or, in one case at least, not bad enough to discontinue treatment. While they all acknowledged that they could not be certain how the course of the disease might have unfolded had they not taken the drug, they generally believed it had been effective for them.
The FDA approved TPOXX as a treatment for smallpox in 2018 based on studies that had infected rabbits with rabbitpox and nonhuman primates with monkeypox. (Smallpox and monkeypox are close viral relatives, so treatments for one are expected to work for the other.) Researchers had to rely on these proxy models of similar viruses because there is no smallpox to investigate, as the virus has been eradicated; and even if there were, it would be unethical to study such a lethal pathogen in humans.
The data indicating the drug is safe for humans comes from a studyof 449 healthy people.
Typically, physicians may use their own judgment to prescribe medications off label for purposes other than those for which they were granted explicit FDA approval.
But given the lack of research on TPOXX’s efficacy in humans, federal health regulations dictate that health care providers may only prescribe the drug for monkeypox through a compassionate-use system overseen by the CDC. Physicians such as Dr. Marshall Glesby, an infectious disease specialist at Weill Cornell Medicine in New York City, said that these strict rules are excessive, including the need to review a more than 100-page treatment-protocol document to qualify as a TPOXX prescriber and to thoroughly document each case.
Dr. Marshall Glesby, an infectious disease specialist at Weill Cornell Medicine in New York City, said the strict rules around prescribing TPOXX are excessive.Benjamin Ryan for NBC News
Such burdens sharply limit the number of health care providers who are willing and able to prescribe TPOXX, according to clinicians who have gained such authority.
“It’s a cumbersome process,” said Dr. Anu Hazra, a physician at Howard Brown Health in Chicago who recently began prescribing the treatment.
“Because we don’t yet know how well this drug is going to work for monkeypox patients,” said Dr. Jennifer McQuiston, who leads the CDC’s monkeypox response, “it is important to ensure we have some data from patients who use it, so we can better understand the risks and benefits and ultimately help other people as well.”
Responding to health care providers’ recent complaints about the TPOXX compassionate-use system, the CDC has, for example, made optional previous requirements that clinicians submit photographs of patients’ monkeypox lesions and ship viral specimens to the agency.
In a July 15 letter to the heads of various federal health agencies, PrEP4All and the nonprofit Partners in Health called on the CDC and FDA to end all restrictions on TPOXX’s use and to allow health care providers to freely prescribe it for monkeypox.
Friday, the CDC announced further revisions to the compassionate-use system, including plans to reduce the 100-plus-page document to under 50; pare back the number of reports physicians must fill out about each patient from six to two; and to permit virtual appointments.
“We have reduced the data we need down to the most critical pieces,” McQuiston said “and have worked to make using this drug simpler, in order to ensure doctors can get the drug to patients who need it.”
Dr. Jason Zucker, an infectious disease specialist at Columbia University Department of Medicine whose team has prescribed the antiviral to 45 patients, said that the U.S. should launch a large randomized clinical trial including people with mild monkeypox disease. If anyone in the placebo arm should progress to severe disease, he proposed, they could be switched into a parallel compassionate-use group. This would not only address the crucial question of the drug’s efficacy but also expand access to treatment while also collecting data on people receiving it in a much more rigorous and organized fashion than he said occurs through the current system.
Jumping through hoops to get TPOXX
Luke Brown said that he first tried to gain access to TPOXX through his primary care provider, who submitted the request to New York City’s health department. The request was denied on the grounds that his case wasn’t serious enough. But then he began to suffer pain so severe all he could do was pace around his apartment for hours; even then, his physician delayed in resubmitting the request. So the well-connected Brown tapped into his contacts on social media and finally found someone who linked him to a local doctor with prescribing authority.
Get the Morning Rundown
Get a head
“It’s infuriating,” he said of the hoops he had to jump through to obtain the drug.
Boomer Banks, an online content creator in New York City, said that he went through a maddening ordeal to obtain TPOXX.Benjamin Ryan for NBC News
“I had to fight for the TPOXX meds,” said an online content creator known as Boomer Banks, also a New Yorker, about what he said was a maddening ordeal finding someone at the city’s health department who could help him access the treatment. “I had no privilege to leverage, just my mouth,” said Banks, who did not want to use his real name used to protect his privacy. “I’m a brown immigrant, 42-year-old HIV-positive sex worker with no insurance. I didn’t take ‘no’ as an answer.”
A recent nonpeer reviewed study posted to a pre-print server found that in laboratory experiments, TPOXX was highly effective at neutralizing the monkeypox strain circulating in the global outbreak.
Under current CDC guidelines, TPOXX is reserved for those with severe disease, including those who are hospitalized or at high risk of a severe outcome because, for example, they are immunocompromised. Those suffering from a common symptom of the virus, intense anorectal or genital pain, qualify for TPOXX, Zucker said.
Brooklyn resident Sebastian Kohn, 39, who had a particularly severe case of monkeypox, said that days after he started TPOXX, the difference in his anorectal pain was “night and day.”
“I can wash myself without wanting to cry,” Kohn said.
Luke Brown holds his bottle of TPOXX pills.Benjamin Ryan for NBC News
Where is the U.S.-based clinical trial?
Asked about the NIH’s plans to back a U.S.-based clinical trial of TPOXX, Judith Hewitt, deputy director of the Office of Biodefense, Research Resources and Translational Research at the National Institute of Allergy and Infectious Diseases, said that “it’s super early days” for such plans.
“There are now just beginning to be discussions about a trial in people living with HIV or at risk of HIV,” she said.
In an email, Dr. Judith Currier, a professor of medicine at the UCLA Division of Infectious Diseases and the chair of a major HIV-related clinical trial network funded by the NIH, confirmed that a trial is being discussed. “I think the holdup is identifying the funding for this work.”
“Money is obviously the real issue here,” Hewitt said. “And so people are scrambling to do what we can do with the resources at hand.” She said the agency is debating whether, for example, to fund a study examining whether a lower dose of the Jynneos vaccine would be highly effective against monkeypox. “So that’s within the same treatment area. But then we’re still up to our eyeballs in Covid.”
Krellenstein, the activist, said, “It’s bizarre, given that we have such large supply in the strategic national stockpile and TPOXX was approved without any human efficacy data, that there weren’t ready-to-go plans for actually doing a U.S. clinical study in the event that we needed to use it.”
According to SIGA’s Hruby, the company might not even look to U.S.trial data on TPOXX to submit to the FDA. Instead, they might rely on the combined findings of the trials already primed to launch in other nations, along with safety data from compassionate-use programs worldwide.
As for how long before the company would submit the drug for FDA approval, Hruby wouldn’t speculate.
“These things always take longer than expected, especially when working with large teams,” Hruby said.
Even on a drug given priority review, the FDA typically takes six months to reach a decision.
TPOXX could help blunt monkeypox’s impact
If approved, TPOXX would offer a future in which the antiviral complements widespread vaccination among at-risk individuals to mitigate monkeypox’s impact on public health, experts said.
The virus could be treated at the very first sign of symptoms, and possibly even during the asymptomatic incubation period if testing technology advances to permit detection at that stage. Such early medical intervention would not only prevent pain and suffering, but would also very likely block transmission of the virus by shortening or eliminating the disease’s infectious period.
Treatment could also save people from the personal and financial hardship of isolating at home for what can be weeks of illness with monkeypox that’s left to resolve on its own.
What’s more, TPOXX could be used as post-exposure prophylaxis among people exposed to monkeypox, either among unvaccinated people or those who cannot be vaccinated, such as the immunocompromised, according to Columbia’s Zucker.
The U.S. Army Medical Research and Development Command does have an established study to assess such a preventive use of this drug. And while a listing of the trial indicates participants must be Department of Defense–affiliated personnel, according to Hruby, there actually is no such restriction.
Friday morning, Luke Brown said his pain had begun to subside and he was watching in wonder as his lesions were steadily sinking back into his skin — “like magic.”
Reflecting on the ordeal monkeypox has been for him, he said it had inspired him to become a public-health activist.
“I’m resolved to see that no one suffers like I did, because no one needs to,” he said.
Anticipating that the U.S. monkeypox outbreak will only continue to expand, he said, “We are just at a crest of avoidable pain unless access to this drug becomes easier.”