Elected officials, nonprofits, activists, and community leaders are pushing forward the idea of safe consumption sites in San Francisco, in order to prevent overdose deaths, improve the health of people who use drugs, and reduce outdoor and public substance use. Safe consumption sites and services are a well-accepted and effective public health intervention that exist in hundreds of cities around the world, but are slow to gain acceptance and be implemented in the U.S.
To gain traction and momentum for safe consumption services in San Francisco, in January Supervisor Hillary Ronen, from San Francisco District 9, organized a panel discussion with a group of experts to share their thoughts on the issue. The event was moderated by Heather Knight from the San Francisco Chronicle, and included Tyler TerMeer, PhD, CEO of San Francisco AIDS Foundation, Alex Kral, PhD, epidemiologist from RTI, Supervisor Matt Dorsey, Dr. Leslie Suen from UCSF, and Sam Rivera, the executive director of OnPoint NYC.
From what I’ve seen, the idea of supervised consumption services can provoke ire from people who don’t know much about the services, how they work, and how they improve the communities in which they exist. People may incorrectly assume they operate as free-for-all, legally-sanctioned, disorganized places that encourage and entice people to use drugs, or maybe enable people in their drug use. This couldn’t be further from the truth.
These are, of course, fears that are based on centuries-old stigma around illicit substance use and addiction, rather than the ample data we now have available from hundreds of sites around the world. The benefits of safe consumption sites are clear: The National Institute of Health shares that safe consumption sites “are associated with lower overdose mortality, 67% fewer ambulance calls for treating overdoses, and a decrease in HIV infections.” We know that safe consumption services increase use of social services–including addiction treatment–and reduce things like public drug use, improper syringe disposal and litter, and public costs spent on HIV/hepatitis C infections, emergency room visits, and overdose.
It was fascinating to hear from Sam Rivera, who is the executive director of OnPoint NYC–the nation’s first supervised consumption centers.
He shared how prior to OnPoint NYC’s opening, the business across from one site had been collecting around 13,000 syringes per month on their own from the surrounding streets. A month after OnPoint opened, that needle waste plummeted to only 1,000 syringes picked up off nearby streets. The site prevented public drug use in the area, which meant far fewer improperly discarded syringes.
NYC’s two sites have also successfully reversed hundreds of overdoses. Rivera talked about how sometimes the percentage of fentanyl in their attendees’ drug-of-choice was so high, people turned blue and started overdosing before they could even complete their injection. Having professionally trained staff on deck to jump in in this crisis situation was essential to saving their lives.
However, if I had to pinpoint the thing that was most notable to me from this panel discussion, it would be something a little less definable, something that doesn’t fit neatly onto a chart or graph to convince funders and politicians of its worthiness. That “X factor” was the unconditional love that was apparent in the way Rivera spoke about people visiting these sites.
As the panel discussion began, Rivera shared a story of a large, six-foot-four man who had come in for injection support. Rivera addressed him by name, and suddenly the man started crying. Rivera, assuming he had used the wrong name or somehow triggered this man’s trauma, apologized profusely. The man explained that Rivera did nothing wrong, he had just not been addressed by his name in such a long time. It was as if hearing his name had, in some inexplicable way, restored a part of his humanity that the streets–and those who so ruthlessly police them–had taken away.
“Just love people,” Rivera explained.
We could feel the authenticity of what Rivera was asserting. “Just love people,” he repeated. Rivera went on to discuss how these sites had unintentionally become a site of bonding–of remembering. “It’s hard to be in those rooms and not get emotional,” he shared. He described how many of the folks working these sites have their own lived experience around substance use, and how their success stories (which include continued use in addition to recovery) serve as a beacon of hope. “We are you,” Rivera said, recalling speaking to a client.
Rivera explained that for some people, safe consumption sites become a place where people explore reducing or ending their substance use. Staff at the site don’t need to constantly ask people about recovery, reducing use, or medication-assisted treatment, Rivera said. Most often, it’s the participants themselves who talk about drug treatment and changing their substance use. As staff get to know the clients who come in, they get to talking. They talk about their interests and their lives. “What we see happen,” Rivera shared, describing these contextual and peripheral conversations while the person is using, “is an [overall] reduction in drug use.”
At the end of the panel discussion, the moderator opened the conversation to audience questions. There were some community members who had shown up in opposition, or at least with extreme doubt in their hearts. They expressed fears that opening a site in San Francisco would attract people who use drugs across the Bay Area, like a lighthouse, cutting through Karl the Fog.
Rivera disputed this idea, sharing that in the year or so they’ve been open, they have not found this to be the case. “Drug users use where they purchase,” Rivera responded, reminding the audience that oftentimes people have an urgency to use, both chemically and also for fear of legal retribution. In NYC, there has been no influx from other areas. He went on to describe how these sites had actually improved relations with local police forces: officers who once indiscriminately arrested people using drugs publicly were now coming to OnPoint NYC in droves to observe and, ultimately, it became evident, to learn.
The question remaining in some audience members’ minds was along the lines of, “What’s your proof that this will work here, in San Francisco, like it has in New York City?” Of course, we won’t actually have definitive proof that it will until we’re able to open a site and measure its impact. But Rivera shared his hope and optimism that San Francisco will be able to implement these life-changing services. “Just be San Francisco,” he said. There was a beat of silence in the room. “Be San Francisco,” he reasserted. “San Francisco always had the gall to step up and do things really radical, really righteous.”
Can we move forward, San Francisco?
Nonprofits across the city are ready to step up and implement these services with City and San Francisco Department of Public health support, something San Francisco AIDS Foundation CEO Dr. Tyler TerMeer emphasized during the panel discussion.
Rivera’s plea to San Franciscans, to remember who we are (or at least once were), reminds me of a segment of the environmental protection movement known as “rewilding.” This form of ecological preservation aims to restore an area’s natural–wild–state. San Francisco has led the nation in many radical movements towards justice–towards love–most notably the gay liberation movement. Perhaps it is time that San Franciscans “rewild” ourselves, restoring our natural, radical roots to effectively address crushing social inequities.
We live in an age in which there is an observable, systemic, systematic callousness towards people who use drugs who may not have housing. The way our society treats folks who use drugs is causing nothing but pain and suffering. Public drug use is at an all-time-high, fatal overdose death rates are through the roof, and incarceration as a response has not worked to solve the issue in any meaningful way. It is time we abandon “tough love” approaches and shift towards something warm. Something radical. Something wild, unimaginable, and powerful. Something loving. We can choose to meet people where they are at–with openness, without judgment, and with unconditional love. Or we can continue down the grim path we’ve been on for decades. We do have a choice.
When Constance Zhou got to college, they noticed that their queer friends were struggling with mental health. But they were also struggling to find providers well-versed in sexual and gender minorities or the complicated intersection of identities that often brought both discrimination and unique therapy needs.
At the same time, Zhou was working at a national suicide hotline, where many of the callers identified as LGBTQ+.
“I was getting people in Texas, in the Midwest, and in the South who really didn’t have access to resources,” Zhou said. “I began to appreciate how important it is to have access to mental health care and that it isn’t one size fits all.”
LGBTQ+ people face unique medical challenges related to sexuality and gender diversity. From experiencing higher rates of mental health stress and substance abuse to requiring gender-affirming care and treatment and prevention of HIV, needs stem from an array of factors related to how the healthcare industry and mainstream culture define identity. The criminalization of gender-affirming care in some states, as well as sports, bathroom, and book bans, contribute to the anguish faced by many in the queer community.
Medical understanding of the needs of queer people has come a long way since 1973 when activists successfully lobbied for the American Psychiatric Association to declassify homosexuality as a mental disorder. Indeed, advancements in health care have been hard fought by the community, often in the face of neglect and hostility by the medical establishment.
The federal government’s failure to respond to the HIV/AIDS crisis in the 1980s and ’90s further galvanized the queer community to take health care into its own hands. Gay Men’s Health Crisis (founded in 1982), the American Foundation for AIDS Research (1985), and ACT UP (1987) were among the early organizations to demand research, innovation, and medical access — efforts that drastically reduced HIV infections and eventually led to effective treatments and medications to prevent the spread of the virus.
Gay Men’s Health Crisis (GMHC) marchers during the annual New York City Pride March on June 30, 1985. Photo by Suzanne Poli/Getty Images
That practice of forcing the medical establishment to address the health needs of the increasingly diverse community is underscored today by efforts to improve gender-affirming care for trans and non-binary people, a movement under attack with 11 states introducing bills to restrict gender-affirming health care access.
“There’s been an enormous amount of harm done to queer people in health care environments,” said David Baker-Hargrove, co-founder and former CEO of 26Health, an LGBTQ+ health care center in Orlando, Florida. “Sometimes, it’s out of willful discrimination, but it’s also from ignorance about how our needs differ and how to interact with and provide services to members of our community.”
Many such issues are systemic, as is the lack of culturally competent care to address the needs of LGBTQ+ people. Demographic differences among queer people also play a determining role in health risks and outcomes, reflecting entrenched social inequalities.
“There are disparities in our community — notably race, ethnicity, and class — that may not be sexuality specific and that drive unequal access to care and prevention services,” Gregg Gonsalves, an early member of ACT UP and today associate professor of epidemiology at Yale School of Public Health, told LGBTQ Nation.
Sexuality and gender identity are among the many considerations included in what the World Health Organization calls social determinants of health — non-medical factors, including economic means and access to education, that impact health risks and outcomes. Such factors account for up to 50 percent of variations in health outcomes in the U.S.
“Addressing social determinants of health is as important as medical interventions,” said Gonsalves, which means addressing factors like access to care is as necessary as developing effective treatment.
That’s where advocates like Zhou come in, with hopes of changing the system for the better. They are determined to help push for care that meets the community’s complex needs by working inside and outside the system for change.
“We’re survivors,” Baker-Hargrove said. “We know how to get along outside of existing systems, and it’s made us strong.”
LGBTQ Nation spoke to a range of queer people who were inspired by their personal experiences to become healthcare advocates and providers.
Constance Zhou co-founded the Weill Cornell Medicine Wellness Qlinic. José Romero advocates for people like themselves who are living with HIV to be part of the solution to ending the epidemic. Dr. Marci Bowers is a pioneering transgender surgeon whose personal experience transitioning informs both her push for innovation and sensitivity toward patients. And Anthony Sorensen was inspired by his own sobriety journey to found Transitional Recovery in Minnesota, which provides LGBTQ+ people in recovery with a supportive living environment.
Constance Zhou: creating new spaces for mental health
Constance Zhou in New York City on December 21, 2022. Photo by Amy Mayes Photography for LGBTQ Nation
Growing up in Charlotte, North Carolina, Constance Zhou, 26, thought mental health was a storm that people weathered on their own.
That changed when Zhou got to college, where they grew comfortable identifying as queer and recognized that many queer people struggle with mental health and seek care, not only for anxiety or depression but for help developing a sense of self and to combat feelings of loneliness.
As a student, Zhou recognized the need for queer-affirming mental health care among their friends, as well as the LGBTQ+ people from around the country who called the suicide hotline where they worked. That led to Zhou’s decision to attend medical school to pursue psychiatry.
After working at a national suicide hotline, Constance Zhou realized the importance of mental health services geared toward the queer community. Photo by Amy Mayes Photography for LGBTQ Nation
Zhou witnessed firsthand the disproportionate mental health stress that young queer people face and the need for more culturally sensitive and affirming providers to meet the demand.
“The issue became very personal to me, being part of the LGBTQ+ community,” Zhou told LGBTQ Nation. “I’m Asian American, queer, and trans. I also identify as nonbinary and use they/them pronouns. And within both the Asian American community and the LGBTQ+ community, there’s a lot of stigma surrounding mental health.”
Parental pressures to succeed in academics, pressure to live up to the “model minority” stereotype, and racial and cultural discrimination are some of the stressors cited in a University of Maryland School of Public Health study. Still, the stigma Zhou mentioned is often a deterrent to seeking help.
Motivated to improve the situation, Zhou decided to specialize in mental health at medical school but said that as a student, they “see that a lot of curricula in medical school really don’t focus on LGBTQ issues.”
Zhou, an M.D./Ph.D. candidate at Weill Cornell Medical College in New York City, co-founded with a classmate the Weill Cornell Medicine Wellness Qlinic, a student-run resource that provides mental health care to queer people while serving as a training ground for the next generation of practitioners.
“I see a lot of patients who are going through feelings and experiences that I have had before,” Zhou said. “Knowing that I can use my own background in understanding and helping them has been very rewarding.”
Co-founding the Wellness Qlinic within the first week of school was transformative. “I never really thought that the work that I did would be meaningful to my queer or trans identity,” Zhou said.
The Wellness Qlinic received immediate support from faculty and administration. “A lot of people went out of their way to make sure that we felt empowered to do what we needed to do,” Zhou said. The clinic, which opened in 2019 and has expanded to include 20 students on the board, functions as a resource for the patients it serves and those who run it.
Student volunteers of Weill Cornell Medicine’s Wellness Qlinic. Photo provided by Weill Cornell Medicine
“Part of the mission of the Wellness Qlinic is to provide free and culturally competent mental health care to queer and trans folks,” Zhou said.
Those services include patient evaluations, individual and group psychotherapy, and medication management. But the clinic also serves as an essential training ground for medical students, residents, and volunteers “to give them the skills they can use later on in their own practice.”
The Wellness Qlinic follows a pattern of similar organizations around the country offering mental health care specifically to queer people. Indeed, the number of clinics offering services specially tailored to LGBTQ+ people decreased by an average of 10 percent each year from 2014 to 2018. As of 2018, about one in five mental health clinics offer services specifically geared toward queer patients.
Nonprofit organizations like Queer LifeSpace, founded in 2011 to offer mental health services to people in the Bay Area regardless of ability to pay, have sprouted up to meet the need. Queer LifeSpace also offers a 12-month clinical training program to help foster the next generation of queer therapists. There are dozens of such clinics around the country. More are necessary to increase access to services for minority populations.
Educating providers is key to improving and expanding health care because, Baker-Hargrove noted, “most health care training programs, no matter the discipline, don’t have a lot of specific training geared towards LGBTQ+ competencies.”
Building community around HIV
José Romero in Raleigh, North Carolina, on December 12, 2022. Photo by Jessica Woodall Photography for LGBTQ Nation
José Romero has also experienced the power of community. As a public health advocate, Romero believes in building networks of mutual support in which people look out for one another. It’s a perspective rooted in personal history and informed by their experience living with HIV and pushing for greater accessibility and education around treatment and prevention.
“I’ve always been around people who have had to find ways to care for each other,” Romero, 30, said. Romero’s family emigrated from an impoverished part of Mexico to rural Washington State, where they worked as farm laborers. The nearest hospital to their small town was such a long drive that Romero’s mother nearly gave birth to them in the car. “I feel like I’ve been mobilizing for health care ever since,” Romero told LGBTQ Nation.
Romero’s first awareness he had been exposed to HIV was a phone call from a doctor.
“I had gone in feeling sick, and he asked me, ‘Do you have sex with men?’ When I said yes, he just immediately shut off to me,” recalled Romero, who identifies as non-binary. “He told me I had been diagnosed with HIV, and I should probably get a follow-up.” Romero made an appointment with another doctor, who was much more supportive.
José Romero in Raleigh, North Carolina. Photo by Jessica Woodall Photography for LGBTQ Nation
Romero didn’t share their diagnosis for another five years when they started working as an organizer. “It’s taken other advocates and people who have lived experience supporting me to get to this point in my life where I’m using my diagnosis for good,” Romero said.
Today, they serve as director of community advocacy, research, and education at Pride Foundation, which gives scholarships to students and funds community organizations serving queer people throughout the Northwest. Pride Foundation was founded in 1985 out of a desire from people dying from HIV/AIDS to leave their money and legacies to benefit the community. Pride Foundation has distributed more than $74 million in grants to queer people and organizations advocating for equity and justice in the decades since.
Since the height of the HIV/AIDS epidemic in the mid-1980s, annual infections in the United States have dropped by more than two-thirds, according to the Centers for Disease Control and Prevention. New HIV infections in the U.S. fell 8 percent from 2015 to 2019. The U.S. Department of Health and Human Services has set a goal of ending the HIV epidemic by 2030, and a number of city-based initiatives with similar aims are underway, including in former epicenters San Francisco and New York.
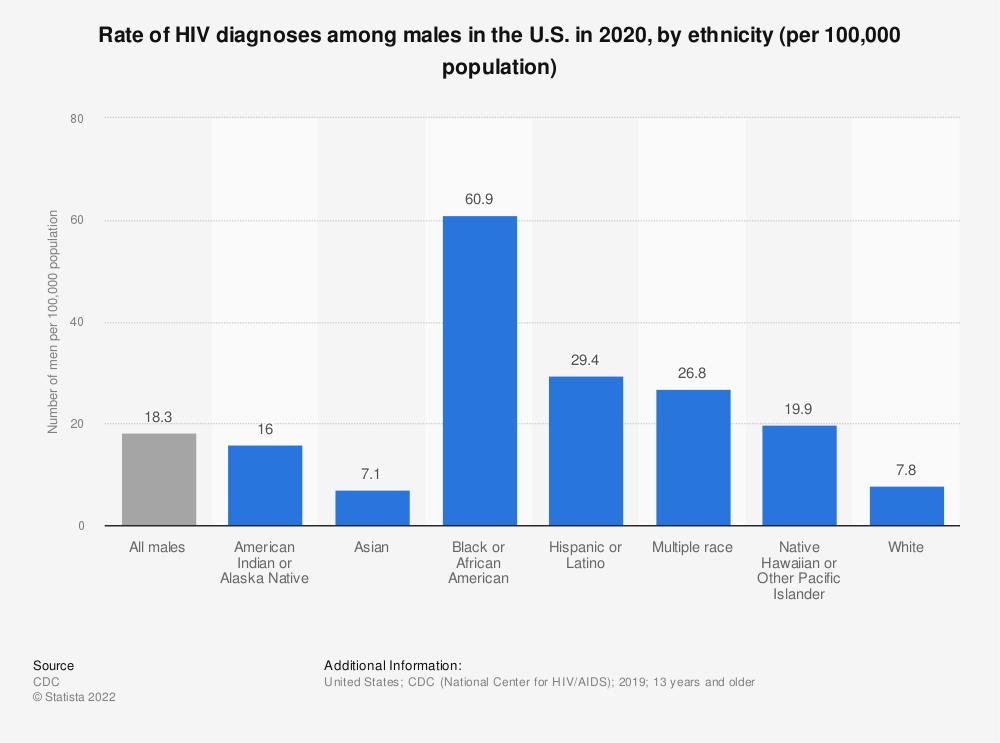
But men who have sex with men account for about 66 percent of new infections each year, despite being only 2 percent of the population, with Black and Latino MSM being affected disproportionately. Each group accounted for around a quarter of new HIV diagnoses among MSM in 2020.
Contributing factors to the high prevalence are intersectional and include racial discrimination, lack of access to resources, language barriers, and stigma. “It’s been really important for me to focus on this big issue by working in coalition and step-by-step,” Romero said. Since they grew up speaking Spanish, Romero recognized language as one of the biggest barriers to healthcare access. They have worked as a translator, interpreter, and advocate for hospitals to provide multilingual materials.
Though medical interventions for the treatment and prevention of HIV, such as antiretrovirals and PrEP, have extended lives and lowered infection rates, advocates are working to improve access for those who need it most, including racial minorities and trans people, who have been underserved by prevention efforts. “It wasn’t until recently that we’ve seen people who are not white or cisgender represented in media around HIV prevention and care,” Romero said.
The medications themselves aren’t enough, Romero said.“We need a social and cultural approach, and that means meaningful involvement of people living with HIV.”
Many factors put people at greater risk of negative health outcomes from HIV, including substance use, mental health, and access to stable housing. Social and political solutions that address these conditions are as important as medical innovations in the fight to end the epidemic.
“Structural interventions in the context of HIV prevention and care are going to need policy-level, community-wide solutions,” Gonsalves said. “This takes us back to the old days of LGBTQ+ advocacy — working to change the sort of environment in which we live to make it easier for us to keep ourselves healthy and safe.”
Half of all new HIV infections are located in the South, where Morris A. Singletary has been working as a peer educator to connect young men of color with care. Based in Atlanta, Singletary, 45, runs the HIV prevention and education initiative PoZitive2PoSitive, offering support and mentorship informed by his lived experience with HIV.
Singletary knows the stakes firsthand. He was near death when he received his HIV diagnosis in 2006, having not understood that he was at risk. And he struggled with the emotional fallout and with adhering to treatment for the next ten years. He also knows the shame, stigma, and lack of awareness that keep men from pursuing care.
“We have to be more intentional,” Singletary said. “We tell people to go to the doctor and get tested, but we don’t say what happens next. We need to show the cycle of care,” he added, including the patient’s role in communicating openly with providers who are trained to show support. Singletary noted that everyone involved in the healthcare process, from researchers and providers to peer educators like himself, has an integral role to play.
Morris Singletary in Atlanta, Georgia. Photo by Seven
“Storytelling is an amazing tool,” Singletary said of the connections he’s forged through sharing his lived experience and encouraging others to seek HIV treatment and prevention.
Romero agrees that people living with HIV should be integral to the path forward, and encourages outreach organizations to hire them to reach others at risk or in need of care. “We need to invest in people to be the solution to the problems that we’re facing,” Romero said. “When we are provided with the resources and opportunity to help each other, we do.”
Dr. Marci Bowers: pioneering gender-affirming healthcare
Dr. Marci Bowers has more than 32 years of experience in pelvic and gynecological surgery. Photo by Drew Bird Photography
Dr. Marci Bowers has devoted much of her history-making career as a surgeon treating transgender people, whose access to essential medical care has come under attack in recent years. Bowers, 64, has performed more than 2,000 vaginoplasties, or bottom surgeries, for trans women and is one of few surgical providers to have undergone the process herself.
“Everyone deserves access to gender-affirming care,” said Bowers, whose medical practice is based in Burlingame, California.
Growing up, Bowers knew she wasn’t comfortable with the gender identity she was assigned at birth, though it was a feeling she couldn’t describe. “I didn’t really have words for what it was to be trans,” Bowers said of the era when there were fewer role models and information. She wound up pursuing medicine, getting married, and having children, playing the role she felt was expected.
“I felt like I could displace my feminine feelings by being a woman’s health care provider,” Bowers said of her decision to become an OB-GYN. It was after Bowers transitioned, at age 37, that she considered pursuing a career in gender-affirmation surgery. “I was responding to an obvious need within the community for more providers,” Bowers said.
Insights gleaned by going through surgery herself have informed her sensitivity toward patients, “not just in the technical aspects of giving them what they want, but recognizing the struggle that they’d already been through being trans.”
Dr. Marci Bowers has performed more than 3,900 gender-affirming surgeries. Studies have shown that gender-affirming surgery is associated with decreased psychological distress, smoking, and suicidal ideation. Photo provided by Dr. Marci Bowers
Trans people experience disproportionately high rates of anxiety and depression and are about six times as likely as the general population to be hospitalized for a suicide attempt. Recentstudies have shown that gender-affirming care, including puberty blockers for trans adolescents, hormone therapy, and potential surgical interventions where necessary, significantly improve mental health and save lives. The latest guidelines from the World Professional Association for Transgender Health advised that hormone treatments can start from age 14.
“It’s an overwhelming, established fact that gender-affirming treatment is effective and greatly enhances psychosocial functioning and reduces suicidality,” Bowers said. “It’s about people improving their lives by assuming the identity that they feel most comfortable with.”
Even as the evidence of efficacy becomes ever more clear, gender-affirming care is being targeted across the country. As of March 2022, 15 states have restricted access to gender-affirming care or are considering laws that would do so. The consequences for people who need care are dire, cutting off access to treatment proven to improve well-being and reduce suicidality.
At the same time, the demand for gender-affirming care is growing, as is the corresponding need for more providers. “It’s growing because people are more comfortable being themselves,” said Bowers, who also helped establish the Transgender Surgical Fellowship Program at Mount Sinai Hospital in New York City to help train more doctors to care for trans people. Under the Affordable Care Act, it’s illegal for insurance providers to deny medically necessary transition-related care, and Bowers also accepts Medicaid from her patients.
“People at every socioeconomic level should have access to this care; we’ve always felt strongly about that,” Bowers said. But even for patients who have coverage, there’s a need for more doctors to provide treatment. “We need more clinicians and mental health professionals to help with the care of this population,” she said.
“Gender identity is a very deeply held value,” Bowers said, an indelible one that requires affirmative care. “It weathers any storm.”
Providing homes for recovery
Richard Fleischman Photography Anthony Sorensen at Gilbert House in Minneapolis, Minnesota, on January 11, 2023. Photo by Rich Fleischman Photography for LGBTQ Nation
When Anthony Sorensen, 52, was growing up on Long Island, New York, his father — who struggled with alcoholism — would disappear for days at a time. When Sorensen was 16, his father left for good, and Sorensen blamed himself, thinking it was because he is gay. Sorensen had started drinking the year before, blacking out the first time he tried alcohol.
“I wanted to be the bad kid who got in trouble in order to feel cool and accepted by my peers,” Sorensen recalled. “But at the same time, to save myself from the humiliation of being called out as gay, I just wanted to disappear.
“The first time I drank, all those fears and inhibitions of being humiliated went away,” Sorensen said.
Feelings of alienation like those Sorensen described are among the reasons that LGBTQ+ people are more than twice as likely to abuse drugs and alcohol than the general population, according to the National Survey on Drug Use and Health, a trend that’s been exacerbated by the coronavirus pandemic. A variety of factors contribute to the increased likelihood, including concurrent mental health conditions like anxiety, depression, and suicidality, themselves often a result of marginalization, discrimination, and trauma.
Drugs and alcohol have also occupied a historically central role in how queer people relate to each other and form social bonds. “Our community was formed in bars,” Baker-Hargrove said. “It can be hard to think about a life within the community that’s not anchored to alcohol or partying.” That’s one reason substance abuse is sometimes normalized within the community, and it may be easier to overlook when someone is struggling.
Sorensen’s heavy drinking and drug use accelerated when he moved to New York City shortly after coming out at age 19. He was 23 when he attended his first Alcoholics Anonymous meeting, but it wasn’t until he discovered AA meetings that were mainly attended by queer people that he was able to work the program and stay sober for two years.
Sorensen’s first experience with Pride Institute, a treatment and recovery center especially focused on the needs of LGBTQ+ people, was in 1999, at a facility in Belle Mead, New Jersey, that has since closed. He stayed sober for 11 years before he began drinking again, when his career as a hairstylist took precedence over his recovery, Sorensen said.
Sorensen later completed two 30-day courses of inpatient treatment at Pride Institute’s main campus in Eden Prairie, Minnesota.
Richard Fleischman Photography Anthony Sorensen at Gilbert House in Minneapolis, Minnesota. Photo by Rich Fleischman Photography for LGBTQ Nation
“Pride 100 percent saved my life,” Sorensen said. “Pride for me was the place where I knew I could authentically be myself without many of the fears that I had carried since I was a kid,” he recalled, noting that he was fortunate to have private insurance and a choice of where to seek treatment. Pride is in-network for most major insurers and works with uninsured patients on lending options to reduce financial barriers to care.
Pride Institute has pioneered a model of treatment specifically tailored to LGBTQ+ people. Since many patients like Sorensen can trace their struggles with addiction back to aspects of their queer identity, centering and affirming those aspects of their lives is essential to effective treatment. “If you can’t totally be yourself, you’re not going to move forward in your recovery,” Sorensen said.
Pride Institute’s affirming environment includes gender-neutral bathrooms and room assignments not based on gender identity assigned at birth, as well as peers and staff with lived experience who embrace and celebrate everyone for who they are. “The counselors are educated in LGBTQ+ issues and addiction and mental illness,” Sorensen said. “They made me sit with my feelings and work through them, rather than escape them” — a process Sorensen called life-changing.
Sorensen also credits the success of his recovery to transitional housing specifically designed for LGBTQ+ people, where those who have completed inpatient programs can live with others in a shared house and offer mutual support. “I saw the success that I had with transitional housing, and I want to be able to reach as many people as possible and give them that same opportunity,” said Sorensen, who ultimately decided to relocate to Minneapolis and dedicate himself to offering queer people in recovery a place to support each other.
A few years into his own recovery, in 2015, Sorensen founded Transitional Recovery in Minnesota (TRIM), which now runs two houses catering to queer people working through addiction. Sorensen works with local outpatient programs, including Pride Institute, which helps subsidize housing costs for patients so that 90 percent of TRIM’s residents have financial support to make the rent accessible.
Richard Fleischman Photography Anthony Sorensen at Gilbert House in Minneapolis, Minnesota. Photo by Rich Fleischman Photography for LGBTQ Nation
“When someone comes into the house, they are 100 percent made to feel like they’re at home,” Sorensen said of TRIM, a model of affirmative support that Sorensen experienced at Pride Institute. “Whether a gay man or a transgender woman who walks through those doors, we all have a very unique set of experiences, but we go through similar things being a minority within our society.”
Though LGBTQ+ people face a variety of challenges based on other aspects of identity and social determinants of health, a sense of solidarity continues to be important in pushing for better health outcomes across the board. “We want everybody to survive, thrive, and prosper,” Gonsalves said, “and LGBTQ+ people need to think of activism as a component of fighting for their health and safety.”
Early activism during the AIDS epidemic continues to be the prime example. Gonsalves pointed to the recent Mpox outbreak and the queer community’s response as proof of how effective collective action continues to be, often in the face of a flawed institutional response.
“LGBTQ+ communities were essential over the past year in slowing down and putting the brakes on the epidemic,” Gonsalves said, noting the pressure placed on government leaders for accelerated vaccine access and the spontaneous reduction of sexual activity that slowed the spread. Unequal risk and access, based on factors like race and class, persisted, and policy-level change is necessary to protect the well-being of the queer community.
In the meantime, LGBTQ+ people continue to lead the charge, taking on disparities the community faces in the medical system and revolutionizing how we care for ourselves and each other.
Transgender youth in Florida will no longer be able to access gender-affirming treatment — even during clinical trials.
The Florida Boards of Medicine and Osteopathic Medicine adopted new rules on Friday banning hormone replacement therapy and puberty blockers for minors.
Also, at a joint meeting of the boards, the Board of Osteopathic Medicine unanimously voided an exception that made it possible for young people to receive medical treatment when enrolled in studies conducted by state universities. This exception resulted from a contentious meeting last year when the two boards voted to have separate standards for different providers when providing gender-affirming medical treatment to minors. As a result, the rules of the two boards are now aligned.
In a Tallahassee hotel where the meeting was held, attendees shouted expletives leading to tense moments that prompted law enforcement officials to position themselves at the front of the room.
“Shame on the Florida Boards of Medicine and Osteopathy for continuing this assault on the health of young people and the rights of their parents to seek the best care possible for their children,” Nikole Parker, director of transgender quality at Equality Florida, said in a statement. “This rule puts transgender youth at higher risk of depression, anxiety, and suicidality and strips parents of the right to make decisions about care for their kids.”
Supporters and advocates pleaded with doctors on the Florida Board of Medicine and the Board of Osteopathic Medicine to retain access to what many described as lifesaving care. One transgender man gave himself a hormone injection during his speaking period. Many spoke of feelings of suicidal ideation passing with access to gender-affirming care.
However, the board was unimpressed and voted in favor of the governor’s ban anyway.
“Those are the facts that have been purposely ignored by Boards of Medicine and Osteopathy stacked with DeSantis allies and campaign donors who have put their toxic politics over people’s health and wellbeing,” Parker said.
“Transgender Floridians exist. Transgender youth exist. Gender-affirming care is lifesaving care — and it is care that is supported by every major medical organization, an overwhelming majority of medical providers, and should be left to young people, their families, and their doctors; not politicians.”
A press conference was held beforehand to condemn the political moves of the Boards and the DeSantis Administration, which attracted more than 150 advocates for transgender and youth rights.
Transgender young people and families whose lives would be affected by the proposed rule spoke at the press event alongside legal experts, medical professionals, and community leaders.
Missouri has launched a multi-agency investigation into a pediatric transgender center after a former case worker alleged children were being routinely prescribed puberty blockers or hormone therapy without “appropriate or accurate” mental health assessments, the state’s attorney general announced Thursday.
Missouri Attorney General Andrew Bailey speaks to reporters after taking the oath of office in Jefferson City on Jan. 3.David A. Lieb / AP
“We have received disturbing allegations that individuals at the Transgender Center at St. Louis Children’s Hospital have been harming hundreds of children each year, including by using experimental drugs on them,” state Attorney General Andrew Bailey said in a statement. “We take this evidence seriously and are thoroughly investigating to make sure children are not harmed by individuals who may be more concerned with a radical social agenda than the health of children.” The investigation was launched two weeks ago after Jamie Reed, who worked as a case manager at the Transgender Center from 2018 to November 2022, alleged the center caused permanent harm to many of the patients being treated for gender dysphoria. The attorney general’s office, which said it had previously received a sworn affidavit and supporting documentation from Reed, confirmed the existence of the investigation Thursday after Reed went public that same day with her allegations in an op-ed published in The Free Press, a news website started by Bari Weiss, a former op-ed writer and editor at The New York Times. Reed concluded her op-ed by calling for a “moratorium on the hormonal and surgical treatment of young people with gender dysphoria.”
In a 23-page affidavit shared on the attorney general’s website, Reed alleged the staff repeatedly violated the center’s own treatment guidelines. She said the center required minors to meet four criteria — a minimum age, a therapist referral, parental consent and a clinical visit with an endocrinologist or an adolescent medicine specialist — before they could receive puberty blockers, which temporarily pause puberty, or hormone therapy, such as estrogen or testosterone. But she alleged the center’s staff would provide the medication “without complete informed parental consent and without an appropriate or accurate assessment of the needs of the child.”
Reed alleged in the affidavit that providers at the center prescribed hormone therapy to patients as young as 13, even though the World Professional Association for Transgender Health, a nonprofit professional association, recommended at the time that minors be at least 16 years old for such treatment. She also alleged providers at the center only used therapists they “knew would say yes” to a patient’s medical transition and that parents were “routinely pressured” into consenting to have their child receive transition-related care.
In her affidavit, Reed also alleged that doctors at the Transgender Center did not share information with patients and their parents about the possibility of sterility following hormone therapy, though, in her op-ed, she said patients were “told about some side effects, including sterility,” but that she “came to believe that teenagers are simply not capable of fully grasping what it means to make the decision to become infertile while still a minor.” She also said she witnessed minors experience “shocking injuries” from the medication, including one patient who experienced “severe atrophy of vaginal tissue” after receiving testosterone and had to have subsequent vaginal lacerations treated surgically.
Reed alleged she raised concerns to doctors at the center and university administrators for years and was discouraged from tracking adverse outcomes of patients, she stated in the affidavit. She wrote in her op-ed that her experience at the Transgender Center has led her to support a nationwide moratorium on gender-affirming care for young people due to “the secrecy and lack of rigorous standards that characterize youth gender transition across the country.”
Washington University in St. Louis, the parent institution of the Children’s Hospital,said in a statement shared on its websiteThursday that it is “alarmed by the allegations reported in the article published by The Free Press describing practices and behaviors the author says she witnessed while employed at the university’s Transgender Center.”
“We are taking this matter very seriously and have already begun the process of looking into the situation to ascertain the facts,” the statement said. “As always, our highest priority is the health and well-being of our patients. We are committed to providing compassionate, family-centered care to all of our patients and we hold our medical practitioners to the highest professional and ethical standards.”
The state’s Division of Professional Registration, one of the agencies assisting in the investigation, is looking into whether any licensed professionals at the Transgender Center are in violation of their respective licensing board’s policies, while the Department of Social Services will be investigating concerns surrounding fraud, waste or abuse in the state’s Medicaid program, according to the attorney general’s news release.
Missouri is one of at least 24 states that have introduced measures this year to prohibit gender-affirming care for minors. Five states — Alabama, Arkansas, Tennessee, Arizona and Utah — have already placed restrictions on such care, though federal courts have blocked Alabama’s and Arkansas’ laws from taking effect pending the outcome of the litigation.
Transition-related care for minors is supported by major medical organizations — including the American Medical Association, the American Academy of Pediatrics and the American Psychological Association. These associations oppose governmental restrictions on care, including puberty blockers and hormone therapy, which they say are safe and have been used for decades to treat other conditions in minors.
The World Professional Association for Transgender Health’s most recent Standards of Care guidance, which is used widely by clinicians who provide transition-related care, recommends that this type of care be provided to minors using a multidisciplinary team of medical experts in a variety of fields, including psychology and endocrinology. The group doesn’t recommend any medical intervention for children prior to puberty. Rather, it recommends that children socially transition, for example, by using a different name and pronouns or wearing a different hairstyle or clothing. Adolescents who begin the early stages of puberty — usually between 8 and 14 — may be eligible for puberty blockers, but the group recommends they meet a list of criteria, including receiving a comprehensive psychosocial assessment.
The group also recommends that older youths meet a list of criteria before beginning hormone therapy. For example, the standards say adolescents have to demonstrate the emotional and cognitive maturity required to provide informed consent for treatment, the adolescent’s other mental health concerns should be addressed, and the adolescent and the parents or guardian should be informed of the potential reproductive effects of the treatment.
Minors rarely receive surgery, but when they do, the group recommends they receive hormone therapy for at least 12 months prior, receive ongoing mental health support and assessments and be informed of the potential health effects of surgery, including infertility.
More than half a dozen studies published in major medical journals over the last few years have found that access to puberty blockers and hormone therapy improves mental health outcomes, including significantly reducing suicidality, for trans youths.
A new study by the Williams Institute at UCLA finds older LGBTQ+ Americans were affected more negatively by the COVID-19 pandemic than their straight peers.
Using data from the U.S. Census Household Pulse Survey, the report examined the demographics, health, and economic experiences of LGBTQ+ adults aged 50 and older during the COVID-19 pandemic.
The study was led by Research Data Analyst Lauren J.A. Bouton, with Amanda M. Brush and Ilan H. Meyer, Distinguished Senior Scholar of Public Policy.
Among the findings:
Almost all LGBTQ+ people over 50 received the COVID-19 vaccine, a higher percentage than their straight peers.
More people aged 50–64 identified as lesbian, gay, bisexual, or transgender than those 65 years of age and older.
More men than women over 50 identified as LGBTQ+, the opposite of younger age groups, where women predominate.
Similar proportions among all LGBTQ+ ethnic groups reported relying on credit cards or loans and savings or retirement to supplement their incomes during the pandemic.
More White LGBTQ+ people reported using the same income sources they used before the pandemic to meet their spending needs.
Reported anxiety and depression numbers during the pandemic were higher among LGBTQ+ individuals than their straight counterparts.
LGBTQ Nation spoke with the study’s lead author to find out what the data reveals and how it can be used to improve the quality of life for a vulnerable population.
LGBTQ NATION: What’s your top-line takeaway from the report?
LAUREN J.A. BOUTON: LGBTQ+ older people, especially older LGBTQ+ people of color, are particularly vulnerable to financial insecurity (food insecurity and housing instability) and health issues such as anxiety and depression symptoms. The vulnerability is compounded by the fact that they don’t have the support many non-LGBTQ+ people have in their lives. For example, they are more likely to live alone, not have children or other supportive family members, and lack LGBTQ+-affirming health care and other services for older people.
LGBTQ NATION: The report states: “Precarity is not new for LGBTQ+ older adults, and COVID-19 may be viewed as part of a continuum of disruptive events that impact the aging experiences of LGBT older adults.” What are some of the other disruptive events that impact aging experiences for older LGBTQ+ adults?
LB: LGBTQ+ older people have had a lifetime of discrimination and stressful events associated with their sexual orientation and gender identity, which research attributes to adverse outcomes. The pandemic is another mechanism by which inequality is perpetuated against the most vulnerable in our society, such as LGBTQ+ older people. Think about how a person with a low income, few resources, and a lack of supportive people around them were facing the pandemic compared with someone who has resources.
LGBTQ NATION: While vaccination rates were higher among LGBTQ+ older adults vs. their straight counterparts, so were mental health issues. Is that a paradox like it sounds? Shouldn’t a vaccination provide peace of mind in addition to protection from the virus?
LB: We don’t know from this report whether vaccination rates and mental health issues are connected. The mental health measures we used were general depression and anxiety symptoms; they did not specifically refer to the pandemic. What we do know is that LGBTQ+ people of all ages experience higher rates of mental health issues, and that was true even before the pandemic. But LGBTQ+ older people also seek mental health treatments, such as prescriptions and therapy, at higher rates, as well. It is plausible that a higher proportion of people getting vaccinated is related to this behavior of being proactive about seeking medical care.
LGBTQ NATION: The report finds a higher percentage of LGBTQ+ older adults reported anxiety and depression symptoms than straight older folks. Is that partly a greater willingness among LGBTQ+ people to speak candidly about mental health than their straight counterparts have? In other words, could you generalize that LGBTQ+ people are more in touch with their feelings?
LB: Minority stress research has demonstrated that people who are discriminated against systemically or individually experience more stress and that stress is related to higher rates of anxiety and depression symptoms, among other health issues. More LGBTQ+ than straight/cisgender people access mental health treatments, which may mean they are more open and honest about their mental health experiences, but we did not test this hypothesis and cannot say to what extent that may be a part of the explanation of the finding about depression and anxiety symptoms.
LGBTQ NATION: The report used the first U.S. Census Bureau data that included questions about sexual orientation and gender identity. How would you describe the impact that had on your study and will have on future LGBTQ+ research?
LB: We applaud the U.S. Census Bureau for including questions that allow us to identify LGBTQ+ people in the dataset. The Household Pulse Survey allows us to make stronger assessments about the experiences of LGBTQ+ people across the nation. The study makes us better able to understand their experiences with food and housing insecurity and we are able to compare these findings to what we’ve already seen in smaller studies. We are hopeful that the Census will continue to add these questions to other surveys such as the American Community Survey, Current Population Survey, and the Decennial Census so we may continue to make progress in understanding the lives and needs of LGBTQ+ people.
Trevor Leopold would have turned 22 on Jan. 30. Instead, he’s “forever 18,” his mother says.
When Greenbrae resident Michelle Leopold received the news that her 18-year-old son died in his Sonoma State University dorm room, she didn’t need to wait for the coroner’s report to know what had killed him.
Although it was November 2019, before most parents had heard of the fentanyl crisis, there was no doubt in Michelle Leopold’s mind that this powerful synthetic opioid was the culprit. Sadly, she was well aware of the dangerous drug because her son’s close friend had succumbed to a fentanyl overdose the previous year.
Indeed, toxicology results confirmed that Trevor Leopold died after ingesting a pill laced with fentanyl. One pill.
He thought he was taking the prescription drug oxycodone, Michelle Leopold said. As it turned out, the fentanyl-laced pill contained no oxycodone at all. Similarly, Trevor Leopold’s friend, who died of a fentanyl overdose in 2018, believed he was consuming Xanax, a prescription benzodiazepine.
“One of the scariest things about this is that so many who end up overdosing don’t know they’re taking something with fentanyl in it,” Dr. Matt Willis, Marin County’s public health director, said in an interview. “It’s kind of like drinking punch that’s been spiked at a party—hard to call it abuse when it’s unintentional. More like a poisoning.”
“There are naive users, who think they’re getting Vicodin or Percocet,” Struzzo said. “They’re not active users and have no tolerance built up for fentanyl. This group has a higher potential for overdose.”
Marin and Sonoma counties, like the rest of the United States, are experiencing a dramatic surge in drug overdoses. Grim statistics reveal the gravity of the crisis, driven by fentanyl.
Overdoses in Marin County have more than doubled since 2018, said Willis. Today, fentanyl is associated with over 50% of OD cases.
The number of fatal ODs in Marin has also increased significantly—more than 100% in the last three years. Every five days, someone dies of an overdose in the county. During 2021 and 2022, 60% of those deaths were linked to fentanyl.
Sonoma County is faring worse, with someone dying every two days from an overdose death, according to the Sonoma County Department of Health. Even more astounding is that deaths involving fentanyl increased by 2,550% from 2016 through 2021.
Exactly how did fentanyl, a powerful legal synthetic opioid developed in 1959, cause this nationwide crisis? Fentanyl, used as an analgesic during surgery and as a prescription drug to treat severe pain, is easily produced and affordable.
Unfortunately, fentanyl’s characteristics also make it attractive to the illicit drug market. In recent years, the supply of fentanyl has grown swiftly, with most of it manufactured outside of the United States. The drug’s effect is similar to heroin, and it’s extremely addictive.
“Fentanyl is up to 100 times more potent than morphine,” Struzzo said.
Drug dealers bank on fentanyl’s addictive quality to keep their customers coming back for more. But just two milligrams of fentanyl—a few grains—can kill a person, according to the Drug Enforcement Agency, which prompted the agency to issue a health alert: “One pill can kill.”
Without access to the sophisticated and expensive scientific weights and measures used by a pharmaceutical company, it’s almost impossible for dealers to calculate how much fentanyl they’re putting into a pill or powder.
And the guy or gal next door may be making those pills, with pill presses for all budgets just a few keystrokes away on Amazon. The presses allow dealers to pump out counterfeit pills that look almost identical to prescription drugs, such as Ritalin, Adderall and oxycodone.
“Fentanyl is now present in most illicit pills and powders,” Willis said. “People overdose from the presence of fentanyl in what’s sold on social media as prescription pills, cocaine or other powders.”
The opioid drug epidemic affects people of all ages, either through intentional or unintentional use. Even infants are brought to emergency rooms with fentanyl ODs.
The issue is daunting and complex; however, Marin and Sonoma have countywide collaboratives to attack the crisis from all sides.
OD Free Marin has five teams, including intervention, treatment and recovery; youth action; education and outreach; equity action; and the justice system. The Sonoma County Prevention Partnership works on drug policy and advocacy efforts.
Both counties agree that a harm reduction approach is beneficial. For example, many pharmacies in Marin and Sonoma sell Narcan, a medication that can reverse the effects of fentanyl, without a prescription. Schools have Narcan, and staff have been trained to administer it. Some experts recommend that every first aid kit contain the life-saving medication. Substance abuse programs are also key to addressing fentanyl use.
Law enforcement agencies are working on getting dealers off the streets, but it can be difficult when social media platforms make it easy for them to hide. For example, Snapchat, a messaging app, allows users to determine how long their messages remain visible. In addition, dealers use different emojis for each drug they have available, negating the need to write anything incriminating.
The illicit drug business, especially with inexpensive fentanyl readily available to dealers, is quite lucrative. There’s always a dealer ready to fill the void when another is arrested, according to Willis.
“Public health and law enforcement agree that we aren’t going to arrest our way out of this problem,” Willis said. “Instead, we partner with the justice system using all of the tools at our disposal, including diverting people with low level drug offenses to assessment and ensuring people who are incarcerated have access to addiction treatment.”
Willis, Struzzo and Michelle Leopold say it’s imperative that people understand the dangers of just one pill.
Leopold plans on educating as many people as possible about what happened to her son, with the goal of preventing fentanyl deaths. “People just don’t know,” she said.
Last year, Leopold and her husband hosted Narcan training sessions at the six Ace Hardware stores they own. Although Leopold admits it’s hard, she makes herself available to the media and speaks at numerous public forums.
“When we got the phone calls about Trevor, I turned to my husband and said, ‘We can’t be quiet about this,’” Leopold said. “There are a lot of us speaking out on behalf of our dead, poisoned children. Hopefully, it’s making a difference.”
Utah is the first state to ban gender-affirming medical care for transgender minors this year.
Gov. Spencer Cox, a Republican, signed a bill Saturday that bars minors from receiving gender-affirming surgeries and places an indefinite moratorium on their access to puberty blockers and hormone therapy.
The bill, which passed in the Utah State Legislature last week, is prospective, so minors who were diagnosed with gender dysphoria before the bill’s effective date, May 3, 2023, would still be able to receive care if they meet a list of requirements.
“Legislation that impacts our most vulnerable youth requires careful consideration and deliberation. While not a perfect bill, we are grateful for Sen. Kennedy’s more nuanced and thoughtful approach to this terribly divisive issue,” Cox said in a statement Saturday, referencing the bill’s sponsor, Republican State Sen. Michael Kennedy. “While we understand our words will be of little comfort to those who disagree with us, we sincerely hope that we can treat our transgender families with more love and respect as we work to better understand the science and consequences behind these procedures.”
In an emotional letter about his veto, Cox cited research about the high risk of suicide among trans youths and additional research that has found that acceptance reduces the risk of suicide.
“I don’t understand what they are going through or why they feel the way they do. But I want them to live,” he wrote. “And all the research shows that even a little acceptance and connection can reduce suicidality significantly.”
But Cox told local news station Fox 13 on Thursday, after the ban on gender-affirming care passed the House, that he did not plan to veto the bill. His office did not immediately return a request for additional comment.
State Sen. Kennedy, a family practice physician, told colleagues in a hearing this month that gender-affirming treatments “lack sufficient long-term research,” according to local radio station KUER.
“But still, our country is witnessing a radical and dangerous push for children to enter this version of health care,” he said.
State Sen. Daniel Thatcher, one of Kennedy’s Republican colleagues, disagreed and was the only Republican to speak out against a previous, though similar, version of the bill, KUER reported. He argued that though he and his colleagues might not understand gender-affirming care, “every credible medical organization on the planet says that that is the safest, best and most appropriate care to save those lives.”
Thatcher added that the bill could face legal challenges because it only prohibits the care for people who are transgender, but it does not prohibit the care for children who might need it for other reasons, KUER reported. The bill provides exemptions for intersex minors, for minors who experience early puberty and for those who have “medically necessary” reasons that don’t include treatment for gender dysphoria.
Thatcher, who is recovering from multiple strokes, was absent from the Senate vote Friday.
A crowd of protestors gathered outside the Utah Capitol on Tuesday ahead of a committee hearing on the bill, during which a number of transgender teens spoke out against it.
Bri Martin, the editor of the student newspaper at West High School, described gender-affirming care as “nothing short of life-saving,” the Salt Lake Tribune reported.
“Me and my family were saved from the arduous and painstaking task of adult transition,” Martin said. “I would like to make clear that no matter the opposition, transitioning was always the only option for me. I deserve a body to feel proud of.”
In addition to barring access to care for minors who don’t already receive it, the legislation also requires the state’s Division of Professional Licensing to create a certification for those who provide hormone treatment to minors. The certification process requires “at least 40 hours of education related to transgender health care for minors from an approved organization,” and providers must obtain this before they can continue to provide such treatment.
It also directs the state’s Department of Health and Human Services to conduct a systematic review of the medical evidence regarding hormonal transgender treatments and provide recommendations to the Legislature, but it does not require the Legislature to review the indefinite moratorium on care after the review is complete.
The measure also allows minors to sue medical providers for malpractice for gender-affirming medical care if the minor “later disaffirms consent” before they turn 25.
Cathryn Oakley, the state legislative director and senior counsel for the Human Rights Campaign, a national LGBTQ advocacy group, condemned the bill last week, just before Cox signed it.
“Utah legislators capitulated to extremism and fear-mongering, and by doing so, shamelessly put the lives and well-being of young Utahans at risk — young transgender folks who are simply trying to navigate life as their authentic selves,” Oakley said, in part, in a statement Friday. “Every parent wants and deserves access to the highest quality health care for our kids.”
Debates over LGBTQ+ rights are having a negative effect on the lives of young people in the community, according to a new poll.
“An overwhelming majority of LGBTQ youth have been negatively impacted by recent debates and laws around anti-LGBTQ policies and that many have also experienced victimization as a result,” says a press release on the poll, conducted for the Trevor Project by Morning Consult between October 23 and November 2 and released this week.
The poll included 716 LGBTQ+ youth ages 13–24 around the U.S. It assessed emotional responses to anti-LGBTQ+ policies as well as which other social issues often give LGBTQ youth stress and anxiety. It came in a year in which more than 220 anti-LGBTQ+ bills were introduced around the nation, most of them targeting transgender youth; many more are being introduced in 2023 — 150 across 23 states in the first two weeks of the year, the Trevor Project reports.
Among the key findings: Eighty-six percent of transgender and nonbinary youth say recent debates about state laws restricting the rights of transgender people have negatively impacted their mental health. A majority of those trans youth (55 percent) said it impacted their mental health “very negatively.” Seventy-one percent of LGBTQ+ youth overall say state laws restricting the rights of LGBTQ+ young people have negatively impacted their mental health.
Seventy-one percent of LGBTQ+ youth — including 82 percent of transgender and nonbinary youth — say that threats of violence against LGBTQ+ spaces, such as community centers, Pride events, drag shows, or medical providers that serve transgender people, often give them stress or anxiety. Nearly half (48 percent) of those LGBTQ+ youth say it gives them stress or anxiety “very often.”
As a result of anti-LGBTQ+ policies and debates in the last year, trans and nonbinary youth say they have had a range of harmful experiences, including cyberbullying or online harassment (45 percent); stopping speaking to a family member (42 percent); not feeling safe going to the doctor or hospital (29 percent); having a friend stop speaking to them (29 percent); bullying at school (24 percent); their school removing Pride flags or other LGBTQ-friendly symbols (15 percent); and physical assault (10 percent).
Among all LGBTQ+ youth, one in three report cyberbullying or online harassment, one in four say they stopped speaking to a family member or relative, and one in five say they experienced bullying.
Regarding policies that will bar doctors from providing gender-affirming medical care to trans and nonbinary youth, 74 percent of these young people say they feel angry, 59 percent feel stressed, 56 percent feel sad, 48 percent feel hopeless, 47 percent feel scared, 46 percent feel helpless, and 45 percent feel nervous.
Policies that prevent trans youth from playing on the sports teams aligned with their gender identity make 64 percent of trans and nonbinary youth feel angry, 44 percent feel sad, 39 percent feel stressed, and 30 percent feel hopeless, according to the poll.
There were also bad reactions to anti-LGBTQ+ school policies, given debates around respecting students’ identities and pronouns, censoring LGBTQ-inclusive curricula, and banning books. New policies that require schools to tell a student’s parent or guardian if they request to use a different name/pronoun or if they identify as LGBTQ+ at school make 67 percent of transgender and nonbinary youth feel angry, 54 percent feel stressed, 51 percent feel scared, 46 percent feel nervous, and 43 percent feel sad.
Fifty-eight percent of LGBTQ+ youth, including 71 percent of transgender and nonbinary youth, feel angry about new policies that bar teachers from discussing LGBTQ+ topics in the classroom. Among trans youth, 59 percent feel sad and 41 percent feel stressed.
Sixty-six percent of LGBTQ+ youth, including 80 percent of transgender and nonbinary youth, feel angry about policies that will ban LGBTQ-inclusive books from school libraries. Nearly half of LGBTQ+ youth, including 54 percent of trans youth, also felt sad about these book bans.
Black LGBTQ+ youth sampled reported disproportionately higher rates of racism, police brutality, doing poorly in school, and gun violence giving them stress or anxiety “very often” compared to white LGBTQ+ youth. Trans and nonbinary youth polled reported disproportionately higher rates of transphobia, losing their health care, anti-LGBTQ+ hate crimes, and threats of violence in LGBTQ+ spaces giving them stress or anxiety “very often” compared to cisgender LGBQ+ youth.
“Right now, we are witnessing the highest number on record of anti-LGBTQ bills introduced this early in any legislative session. We must consider the negative toll of these ugly public debates on youth mental health and well-being. LGBTQ young people are watching, and internalizing the anti-LGBTQ messages they see in the media and from their elected officials. And so are those that would do our community harm,” Kasey Suffredini, vice president of advocacy and government affairs at the Trevor Project, said in the release.
Suffredini added: “The Trevor Project is proud to see that more than two-thirds of LGBTQ youth, including 81 percent of transgender and nonbinary youth, have seen, read, or heard about our work to fight back against anti-LGBTQ bills. We are prepared for the fight ahead and will not stop advocating for a safer, more accepting world for all.”
Republican Florida Gov. Ron DeSantis is asking state universities for the number and ages of their students who sought or received gender dysphoria treatment, including sex reassignment surgery and hormone prescriptions, according to a survey released Wednesday.
Why he’s conducting the survey wasn’t completely clear. DeSantis has been criticized by LGBTQ advocates for policies seen as discriminatory, including banning instruction on sexual and gender identity in early grades and making it easier for parents to remove books related to the topic in public schools.
“We can see cuts in funding for universities to treat students with this condition, and I think an all-out elimination of services is certainly on the table,” said House Democratic Leader Fentrice Driskell.
The survey was released the same day the university presidents voted to support DeSantis’ anti-woke agenda and to reject “the progressivist higher education indoctrination agenda” and committing to “removing all woke positions and ideologies by February 1, 2023,” according to a Department of Education news release.
The survey is being sent to the university board of trustee chairs by DeSantis’ budget director, Chris Spencer.
“Our office has learned that several state universities provide services to persons suffering from gender dysphoria,” Spencer wrote. “On behalf of the Governor, I hereby request that you respond to the enclosed inquiries related to such services.”
The governor’s office did not respond to emails and a phone call seeking information about the purpose of the survey, which must be completed by Feb. 10. Spencer told the chairs the survey is to be completed as part of their obligation to govern institutional resources and protect the public interest.
Driskell said DeSantis is trying to remake the state’s universities “in his own image” as far as what can be taught and how students can be treated.
“I’ve never seen anything like this. It’s a really terrifying place that we’re at in Florida history,” Driskell said. “What can happen is a brain drain where we have Florida students not want to stay here and attend school at our public colleges and universities.”
The survey is similar to one the governor is forcing state universities to complete regarding spending on diversity, equity and inclusion and critical race theory programs.
The current memo asks universities to “provide the number of encounters for sex-reassignment treatment or where such treatment was sought” as well as data for students referred to other facilities. It says to protect students’ identities when completing the information.
The survey requires a breakdown by age, regardless of whether the student is age 18 or older, of people prescribed hormones or hormone antagonists or who underwent a medical procedures like mastectomies, breast augmentation or removal and reconstruction of genitals.
Far-right pundit Jordan Peterson has finally discovered that his actions have consequences following several controversial tweets.
The anti-LGBTQ+ author has been told he could have his psychology licence revoked if he refuses to undergo a mandatory coaching program by the College of Psychologists of Ontario (CPO).
Peterson initially revealed he was obligated to take the course in a 3 January twitter thread.
“The Ontario College of Psychologists has demanded that I submit myself to mandatory social media communication retraining with their experts,” he wrote.
“About a dozen people from all over the world submitted complaints about my public statements on Twitter and [The Joe Rogan Podcast] over a four-year period claiming I had ‘harmed’ people with my views.”
The former Toronto psychology professor also aired his frustrations at the obligatory media training course in a 4 January column for The National Post.
He cited his tweets criticising Canadian president Justin Trudeau – for what he described as an “unconstitutional” COVID-19 travel ban, while also calling him a “puppet” – as the reason for the admonishment from the Ontario College of Psychologists.
“What exactly have I done that is so seriously unprofessional that I am now a danger not only to any new potential clients but to the public itself?” Peterson wrote.
Jordan Peterson has claimed his tweets criticising Justin Trudeau were predominantly why he is obligated to attend the media training session. (Getty)
Others have routinely cited his often blatantly anti-LGBTQ+ tweets and rhetoric, including claims that being trans is a “contagion” similar to “satanic ritual abuse”.
Peterson acknowledged these criticisms in his column, saying that he had been labelled “sexist, transphobic” and a “climate change denialist”.
Despite the plethora of examples detailing Peterson’s vehement anti-LGBTQ+ sentiments – including several dozen tweets and audio snippets of him comparing the trans community to “borderline schizophrenic” individuals – he failed to cite any in his article.
Most notable was his refusal to correctly gender actor Elliot Page in a set of tweets in July, prompting his several-month-long ban from Twitter before being reinstated after Elon Musk’s acquisition of the site.
After being banned, Peterson recorded a 15-minute YouTube video titled “Twitter ban” which saw the media pundit call gender-affirming healthcare a “viciously harmful fad”.
Since being reinstated, Peterson’s rhetoric against the transgender and LGBTQ+ community has continued among his repeated tweets of lockdown scepticism and far-right ideological rhetoric.
In a statement to Global News, the CPO said: “The college is not authorised to discuss this matter as per the confidentiality provisions of section 36 of Ontario’s Regulated Health Professions Act, 1991.”